Memory Clinic, Department of Neurology, Second Faculty of Medicine, Charles University and Motol University Hospital, Prague, 15006, Czech Republic.
Division of Clinical Geriatrics, Centre for Alzheimer Research, Department of Neurobiology, Care Sciences, and Society, Karolinska Institutet, Stockholm, 14183, Sweden.
Alzheimers Res Ther. 2024 Jul 5;16(1):153. doi: 10.1186/s13195-024-01517-5.
Alzheimer's disease (AD) is a progressive neurodegenerative disorder where pathophysiological changes begin decades before the onset of clinical symptoms. Analysis of brain atrophy patterns using structural MRI and multivariate data analysis are an effective tool in identifying patients with subjective cognitive decline (SCD) at higher risk of progression to AD dementia. Atrophy patterns obtained from models trained to classify advanced AD versus normal subjects, may not be optimal for subjects at an early stage, like SCD. In this study, we compared the accuracy of the SCD progression prediction using the 'severity index' generated using a standard classification model trained on patients with AD dementia versus a new model trained on β-amyloid (Aβ) positive patients with amnestic mild cognitive impairment (aMCI).
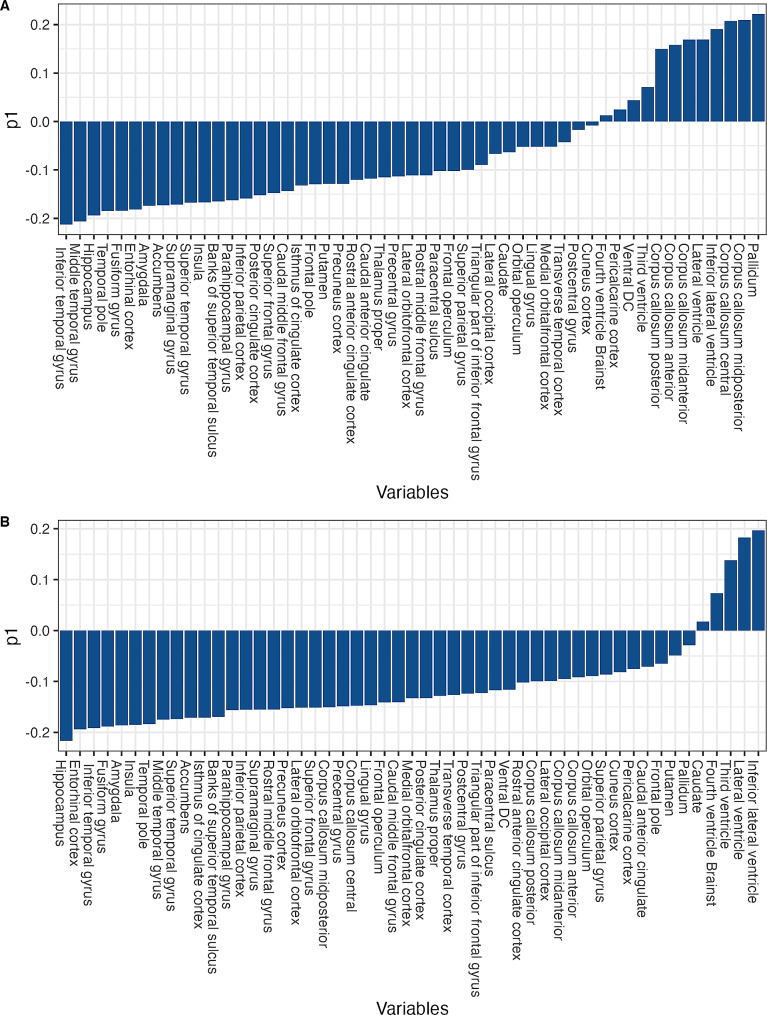
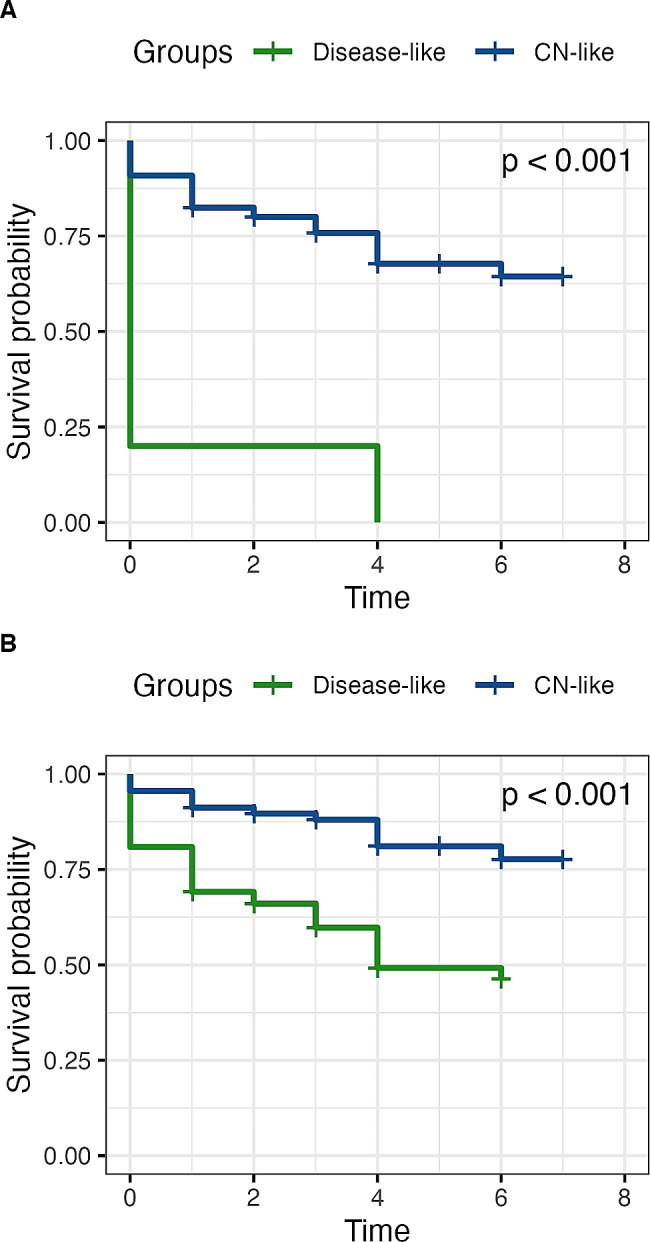
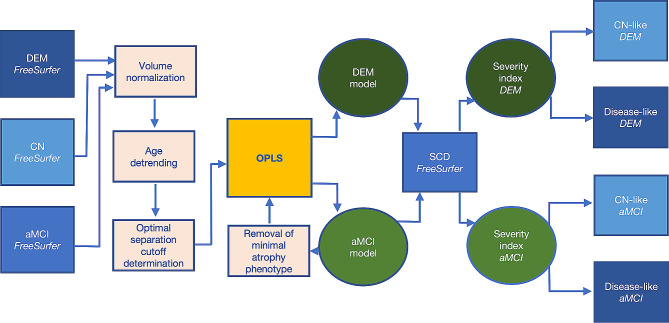
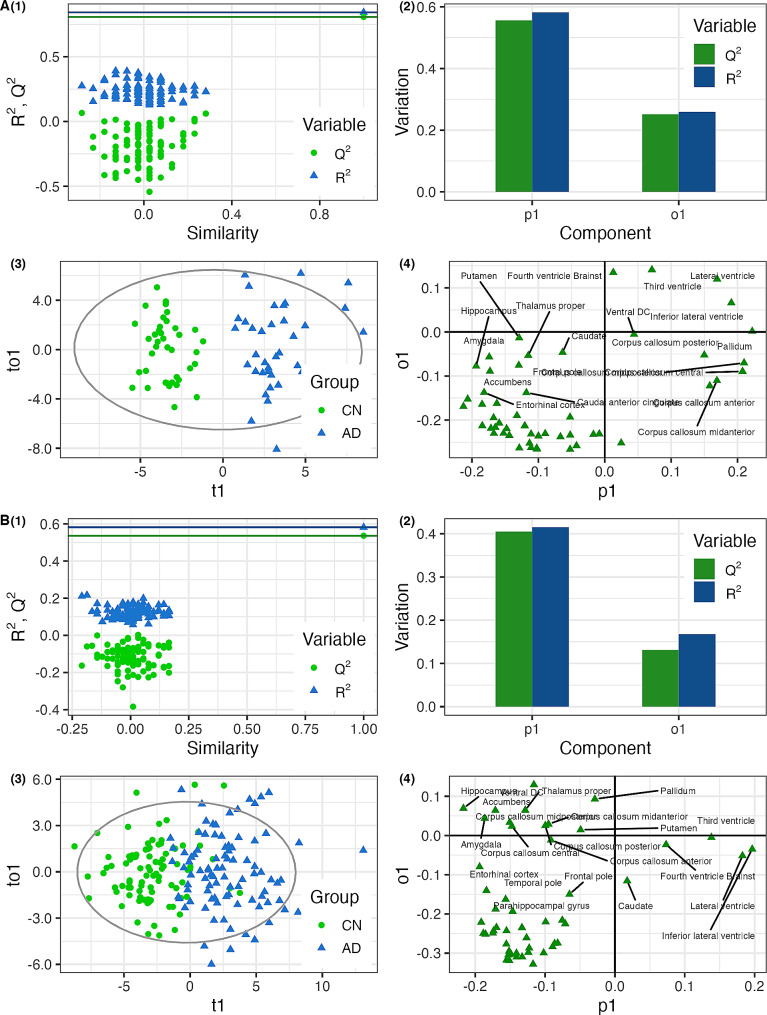
We used structural MRI data of 504 patients from the Swedish BioFINDER-1 study cohort (cognitively normal (CN), Aβ-negative = 220; SCD, Aβ positive and negative = 139; aMCI, Aβ-positive = 106; AD dementia = 39). We applied multivariate data analysis to create two predictive models trained to discriminate CN individuals from either individuals with Aβ positive aMCI or AD dementia. Models were applied to individuals with SCD to classify their atrophy patterns as either high-risk "disease-like" or low-risk "CN-like". Clinical trajectory and model accuracy were evaluated using 8 years of longitudinal data.
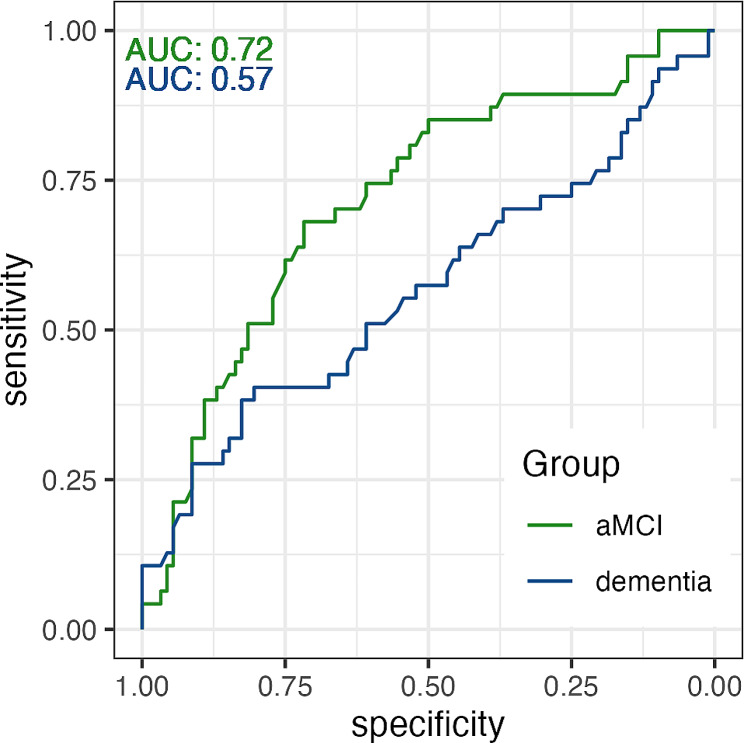
In predicting progression from SCD to MCI or dementia, the standard, dementia-based model, reached 100% specificity but only 10.6% sensitivity, while the new, aMCI-based model, reached 72.3% sensitivity and 60.9% specificity. The aMCI-based model was superior in predicting progression from SCD to MCI or dementia, reaching a higher receiver operating characteristic area under curve (AUC = 0.72; P = 0.037) in comparison with the dementia-based model (AUC = 0.57).
When predicting conversion from SCD to MCI or dementia using structural MRI data, prediction models based on individuals with milder levels of atrophy (i.e. aMCI) may offer superior clinical value compared to standard dementia-based models.
阿尔茨海默病(AD)是一种进行性神经退行性疾病,其病理生理变化在临床症状出现前几十年就开始了。使用结构 MRI 和多变量数据分析来分析脑萎缩模式是识别有主观认知下降(SCD)风险更高的患者进展为 AD 痴呆的有效工具。从针对 AD 痴呆与正常受试者进行分类的模型中获得的萎缩模式,可能并不适合处于早期阶段的患者,如 SCD。在这项研究中,我们比较了使用基于 AD 痴呆患者训练的标准分类模型生成的“严重程度指数”和基于β-淀粉样蛋白(Aβ)阳性遗忘型轻度认知障碍(aMCI)患者训练的新模型对 SCD 进展预测的准确性。
我们使用了瑞典 BioFINDER-1 研究队列的 504 名患者的结构 MRI 数据(认知正常(CN),Aβ 阴性=220;SCD,Aβ 阳性和阴性=139;aMCI,Aβ 阳性=106;AD 痴呆=39)。我们应用多变量数据分析创建了两个预测模型,用于区分 CN 个体与 Aβ 阳性 aMCI 或 AD 痴呆患者。将模型应用于 SCD 个体,将其萎缩模式分类为高风险“疾病样”或低风险“CN 样”。使用 8 年的纵向数据评估临床轨迹和模型准确性。
在预测 SCD 向 MCI 或痴呆进展方面,基于痴呆的标准模型达到了 100%的特异性,但只有 10.6%的敏感性,而基于 aMCI 的新模型达到了 72.3%的敏感性和 60.9%的特异性。基于 aMCI 的模型在预测 SCD 向 MCI 或痴呆进展方面表现更优,与基于痴呆的模型相比,其获得的更高的接收器工作特征曲线下面积(AUC=0.72;P=0.037)。
使用结构 MRI 数据预测 SCD 向 MCI 或痴呆的转化时,基于较轻萎缩程度的个体(即 aMCI)的预测模型可能比基于痴呆的标准模型具有更高的临床价值。