Department of Statistics and Quantitative Methods, Unit of Biostatistics, Epidemiology and Public Health, University of Milano-Bicocca, Via Bicocca Degli Arcimboldi, 8, Milan, 20126, Italy.
National Centre for Healthcare Research and Pharmacoepidemiology, University of Milano-Bicocca, Milan, Italy.
BMC Public Health. 2024 Jul 6;24(1):1808. doi: 10.1186/s12889-024-19346-4.
Single-pill combination (SPC) of three antihypertensive drugs has been shown to improve adherence to therapy compared with free combinations, but little is known about its long-term costs and health consequences. This study aimed to evaluate the lifetime cost-effectiveness profile of a three-drug SPC of an angiotensin-converting enzyme inhibitor, a calcium-channel blocker, and a diuretic vs the corresponding two-pill administration (a two-drug SPC plus a third drug separately) from the Italian payer perspective.
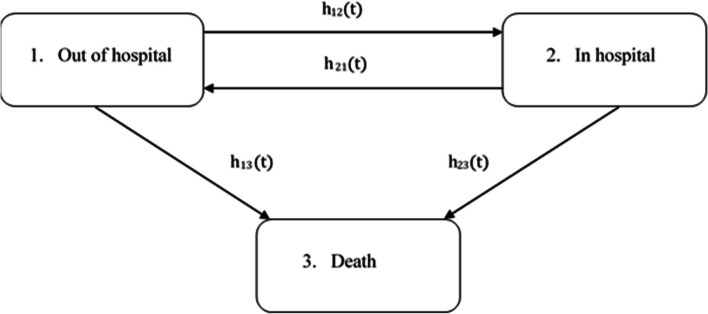
A cost-effectiveness analysis was conducted using multi-state semi-Markov modeling and microsimulation. Using the healthcare utilization database of the Lombardy Region (Italy), 30,172 and 65,817 patients aged ≥ 40 years who initiated SPC and two-pill combination, respectively, between 2015 and 2018 were identified. The observation period extended from the date of the first drug dispensation until death, emigration, or December 31, 2019. Disease and cost models were parametrized using the study cohort, and a lifetime microsimulation was applied to project costs and life expectancy for the compared strategies, assigning each of them to each cohort member. Costs and life-years gained were discounted by 3%. Probabilistic sensitivity analysis with 1,000 samples was performed to address parameter uncertainty.
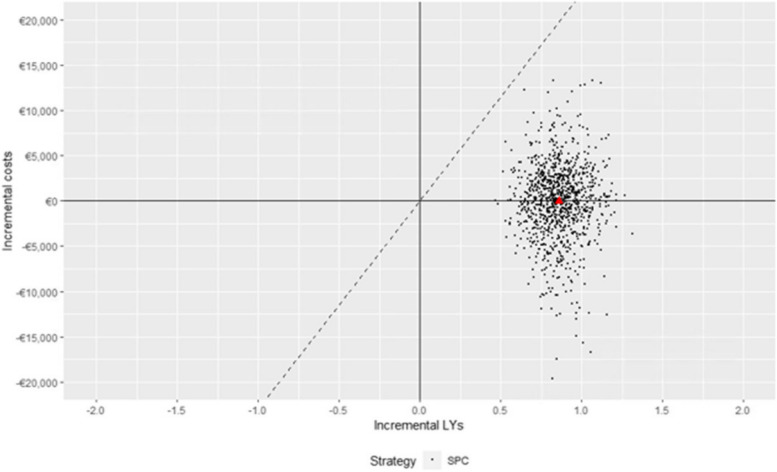
Compared with the two-pill combination, the SPC increased life expectancy by 0.86 years (95% confidence interval [CI] 0.61-1.14), with a mean cost differential of -€12 (95% CI -9,719-8,131), making it the dominant strategy (ICER = -14, 95% CI -€15,871-€7,113). The cost reduction associated with the SPC was primarily driven by savings in hospitalization costs, amounting to €1,850 (95% CI 17-7,813) and €2,027 (95% CI 19-8,603) for patients treated with the SPC and two-pill combination, respectively. Conversely, drug costs were higher for the SPC (€3,848, 95% CI 574-10,640 vs. €3,710, 95% CI 263-11,955). The cost-effectiveness profile did not significantly change according to age, sex, and clinical status.
The SPC was projected to be cost-effective compared with the two-pill combination at almost all reasonable willingness-to-pay thresholds. As it is currently prescribed to only a few patients, the widespread use of this strategy could result in benefits for both patients and the healthcare system.
与自由联合治疗相比,三药单片复方(SPC)已被证明能提高治疗依从性,但对于其长期成本和健康后果知之甚少。本研究旨在从意大利支付者的角度评估血管紧张素转换酶抑制剂、钙通道阻滞剂和利尿剂三药 SPC 与相应的两药给药(两药 SPC 加第三种药物单独给药)的终生成本效益情况。
使用多状态半马尔可夫模型和微模拟进行成本效益分析。使用伦巴第大区(意大利)的医疗保健利用数据库,确定了 2015 年至 2018 年期间分别开始服用 SPC 和两药组合的≥40 岁患者 30172 名和 65817 名。观察期从首次药物配药开始,持续到死亡、移民或 2019 年 12 月 31 日。使用研究队列对疾病和成本模型进行参数化,并应用终生微模拟为比较策略预测成本和预期寿命,为每个队列成员分配每种策略。成本和获得的生命年以 3%贴现。进行了 1000 次样本的概率敏感性分析以解决参数不确定性。
与两药组合相比,SPC 使预期寿命延长了 0.86 年(95%置信区间[CI]0.61-1.14),平均成本差异为-€12(95%CI-9,719-8,131),使其成为主导策略(ICER=-14,95%CI-€15,871-€7,113)。SPC 相关的成本降低主要是由于住院费用的节省,SPC 治疗的患者节省了€1850(95%CI17-7813)和€2027(95%CI19-8603),而两药组合治疗的患者节省了€1850(95%CI17-7813)和€2027(95%CI19-8603)。而 SPC 的药物成本较高(€3848,95%CI574-10640 比 €3710,95%CI263-11955)。成本效益状况在几乎所有合理的意愿支付阈值下均未随年龄、性别和临床状况的不同而显著改变。
与两药组合相比,SPC 预计具有成本效益。由于它目前仅用于少数患者,因此广泛使用这种策略可能会使患者和医疗保健系统都受益。