Forte Research (Pty ltd) and Private Practice South Africa, Pretoria, South Africa.
Instituto do Coração, Hospital das Clinicas-FMUSP, São Paulo, Brazil.
J Hypertens. 2024 Jan 1;42(1):136-142. doi: 10.1097/HJH.0000000000003570. Epub 2023 Sep 19.
This analysis compared adherence, cardiovascular (CV) events and all-cause mortality incidence, and healthcare costs among hypertensive patients treated with perindopril (PER)/indapamide (IND)/amlodipine (AML) in single-pill combination (SPC) vs. multiple-pill combination, in a real-world setting in Italy.
In this observational retrospective analysis of Italian administrative databases, adult patients treated with PER/IND/AML between 2010 and 2020 were divided into two cohorts: single-pill vs. multiple-pill. Patient data were available for at least one year before and after index date. Propensity score matching (PSM) was applied to reduce selection bias. Adherence was defined as proportion of days covered: non-adherence, <40%; partial adherence, 40-79%, and adherence ≥80%. Mortality incidence and CV events as single, or composite, endpoints were evaluated after first year of follow-up. Healthcare cost analyses were performed from the perspective of the Italian National Health Service.
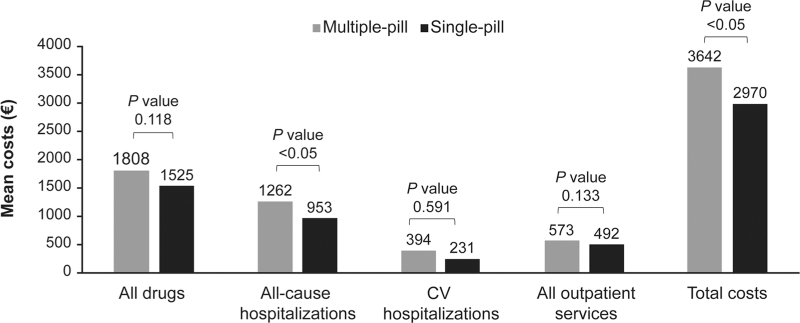
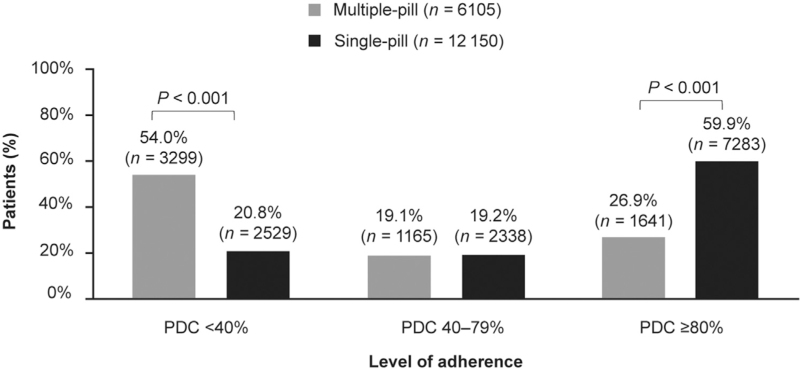
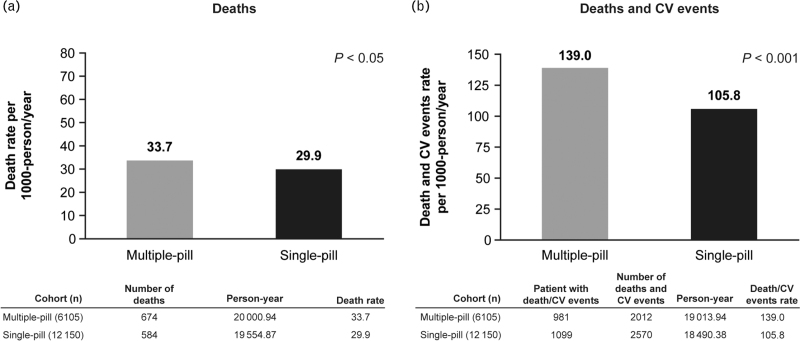
Following PSM, the single-pill cohort included 12 150 patients, and the multiple-pill cohort, 6105. The SPC cohort had a significantly higher percentage of adherent patients vs. the multiple-pill cohort (59.9% vs. 26.9%, P < 0.001). Following the first year of follow-up, incidence of all-cause mortality, and combined endpoint of all-cause mortality and CV events were lower in the SPC cohort compared with multiple-pill cohort. Average annual direct healthcare costs were lower in the single-pill cohort (€2970) vs. multiple-pill cohort (€3642); cost of all drugs and all-cause hospitalizations were major contributors.
The SPC of PER/IND/AML, compared with multiple-pill combination, is associated with higher adherence to medication, lower incidence of CV events and mortality, and reduced healthcare costs.
本分析比较了意大利真实环境中,使用培哚普利/吲达帕胺/氨氯地平单片复方制剂(SPC)与多片复方制剂治疗的高血压患者的依从性、心血管(CV)事件和全因死亡率发生率以及医疗保健成本。
在这项对意大利行政数据库的观察性回顾性分析中,将 2010 年至 2020 年间接受培哚普利/吲达帕胺/氨氯地平治疗的成年患者分为单片剂和多片剂两组。患者在指数日期前后至少有一年的可用数据。应用倾向评分匹配(PSM)来减少选择偏倚。依从性定义为覆盖率天数的比例:不依从,<40%;部分依从,40-79%,依从性≥80%。在随访的第一年之后,评估了死亡率和 CV 事件作为单一或复合终点的发生率。从意大利国家卫生服务的角度进行了医疗保健成本分析。
在 PSM 之后,单片剂队列包括 12150 名患者,多片剂队列包括 6105 名患者。与多片剂队列相比,SPC 队列的依从性患者比例显著更高(59.9%比 26.9%,P<0.001)。在随访的第一年之后,SPC 队列的全因死亡率和全因死亡率和 CV 事件复合终点的发生率均低于多片剂队列。单片剂队列的年平均直接医疗保健成本(€2970)低于多片剂队列(€3642);所有药物和全因住院治疗的费用是主要贡献因素。
与多片复方制剂相比,培哚普利/吲达帕胺/氨氯地平 SPC 与更高的药物依从性、更低的 CV 事件和死亡率发生率以及降低的医疗保健成本相关。