Schaefer Jordan K, Errickson Josh, Kong Xiaowen, Ali Mona A, DeCamillo Deborah, Edupuganti Subhash, Haymart Brian, Kaatz Scott, Kline-Rogers Eva, Kozlowski Jay H, Krol Gregory D, Sood Suman L, Froehlich James B, Barnes Geoffrey D
Division of Hematology/Oncology, Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan, USA.
Consulting for Statistics, Computing, and Analytics Research, University of Michigan, Ann Arbor, Michigan, USA.
Res Pract Thromb Haemost. 2024 May 24;8(4):102449. doi: 10.1016/j.rpth.2024.102449. eCollection 2024 May.
For patients anticoagulated with direct oral anticoagulants (DOACs) or warfarin and on aspirin (ASA) for nonvalvular atrial fibrillation and/or venous thromboembolism, it is unclear if bleeding outcomes differ.
To assess bleeding rates for ASA with DOACs vs warfarin and one another.
Registry-based cohort study of patients followed by a 6-center quality improvement collaborative in Michigan using data from 2009 to 2022. The study included adults on ASA with warfarin or DOACs for atrial fibrillation and/or venous thromboembolism without a recent myocardial infarction or heart valve replacement.
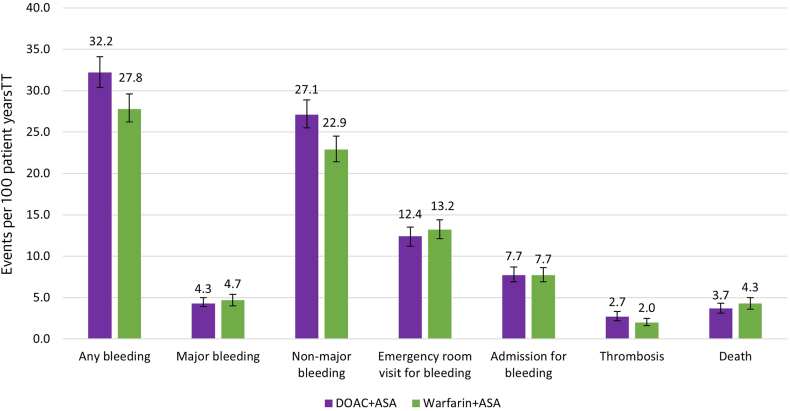
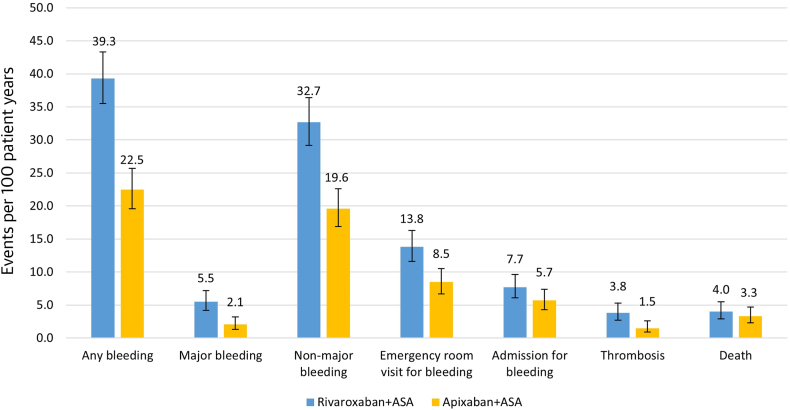
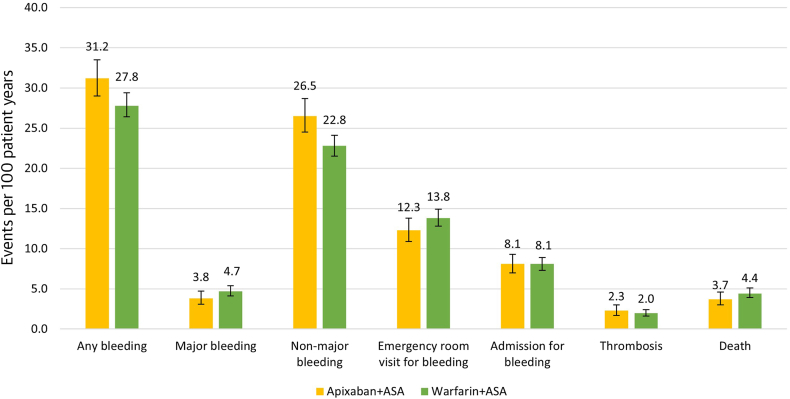
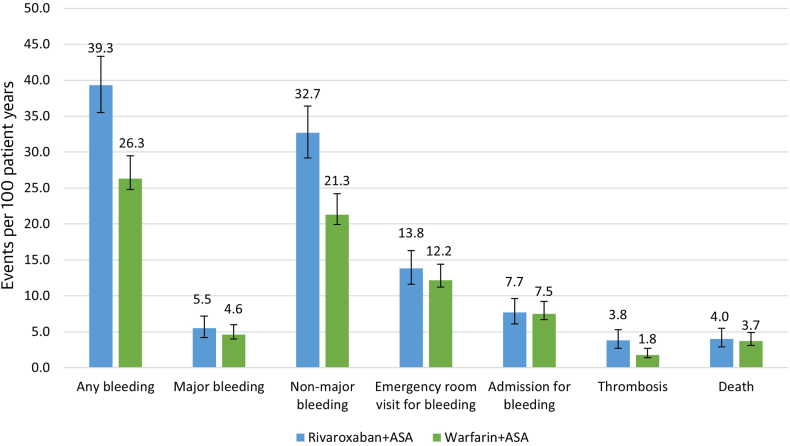
After propensity matching by anticoagulant class, we compared 2 groups of 1467 patients followed for a median of 18.0 months. Any bleeding and nonmajor bleeding was increased with DOACs + ASA compared with warfarin + ASA (32.2 vs 27.8 and 27.1 vs 22.9 events/100 patient-years; relative risks [RRs], 1.1 and 1.2; 95% CIs, 1.1-1.2 and 1.1-1.3, respectively). After matching by drug, patients on apixaban + ASA vs warfarin + ASA had more bleeding (31.2 vs 27.8 events/100 patient-years; RR, 1.1; 95% CI, 1.0-1.2) and nonmajor bleeding but less major bleeding (3.8 vs 4.7 events/100 patient-years; RR, 0.8; 95% CI, 0.6-1.0) and emergency room visits for bleeding. Patients on rivaroxaban + ASA vs warfarin + ASA had more bleeding (39.3 vs 26.3 events/100 patient-years, RR, 1.5; 95% CI, 1.3-1.6), nonmajor bleeding, and thrombosis. Patients on apixaban + ASA vs rivaroxaban + ASA had significantly less bleeding (22.5 vs 39.3/100 patient-years; RR, 0.6; 95% CI, 0.5-0.7), nonmajor bleeding, major bleeding (2.1 vs 5.5 events/100 patient-years; RR, 0.4; 95% CI, 0.2-0.6), emergency room visits for bleeding, and thrombotic events.
Patients on DOAC + ASA without a recent myocardial infarction or heart valve replacement had more nonmajor bleeding but otherwise similar outcomes compared with warfarin + ASA. Patients treated with rivaroxaban + ASA experienced more adverse clinical events compared with warfarin + ASA or apixaban + ASA.
对于使用直接口服抗凝剂(DOACs)或华法林抗凝且服用阿司匹林(ASA)治疗非瓣膜性心房颤动和/或静脉血栓栓塞的患者,出血结局是否存在差异尚不清楚。
评估DOACs联合ASA与华法林联合ASA以及两者之间的出血率。
基于注册研究的队列研究,对密歇根州一个由6个中心组成的质量改进协作组在2009年至2022年期间随访的患者进行研究。该研究纳入了因心房颤动和/或静脉血栓栓塞服用华法林或DOACs及ASA且近期无心肌梗死或心脏瓣膜置换术的成年人。
按抗凝剂类别进行倾向评分匹配后,我们比较了两组各1467例患者,中位随访时间为18.0个月。与华法林+ASA相比,DOACs+ASA的任何出血和非大出血事件增加(分别为32.2 vs 27.8以及27.1 vs 22.9事件/100患者年;相对风险[RRs]分别为1.1和1.2;95%置信区间[CIs]分别为1.1 - 1.2和1.1 - 1.3)。按药物匹配后,阿哌沙班班+ASA组与华法林+ASA组相比有更多出血(31.2 vs 27.8事件/100患者年;RR,1.1;95%CI,1.0 - 1.2)和非大出血,但大出血较少(3.8 vs 4.7事件/100患者年;RR,0.8;95%CI,0.6 - 1.0)以及因出血的急诊就诊次数。利伐沙班+ASA组与华法林+ASA组相比有更多出血(39.3 vs 26.3事件/100患者年,RR,1.5;95%CI,1.3 - 1.6)、非大出血和血栓形成。阿哌沙班+ASA组与利伐沙班+ASA组相比有显著更少的出血(22.5 vs 39.3/100患者年;RR,0.6;95%CI,0.5 - 0.7)、非大出血、大出血(2.1 vs 5.5事件/100患者年;RR,0.4;95%CI,0.2 - 0.6)、因出血的急诊就诊次数和血栓形成事件。
近期无心肌梗死或心脏瓣膜置换术的DOAC+ASA患者有更多非大出血,但与华法林+ASA相比其他结局相似。与华法林+ASA或阿哌沙班+ASA相比,利伐沙班+ASA治疗的患者经历了更多不良临床事件。