Silveira-Freitas Jayme Euclydes Picasky, Campagnolo Maria Luiza, Dos Santos Cortez Mariana, de Melo Fabrício Freire, Zarpelon-Schutz Ana Carla, Teixeira Kádima Nayara
Campus Toledo, Universidade Federal do Paraná, Toledo, Paraná 85919-899, Brazil.
Instituto Multidisciplinar em Saúde, Universidade Federal da Bahia, Campus Anísio Teixeira, Vitória da Conquista, Bahia 45029-094, Brazil.
World J Virol. 2024 Jun 25;13(2):89985. doi: 10.5501/wjv.v13.i2.89985.
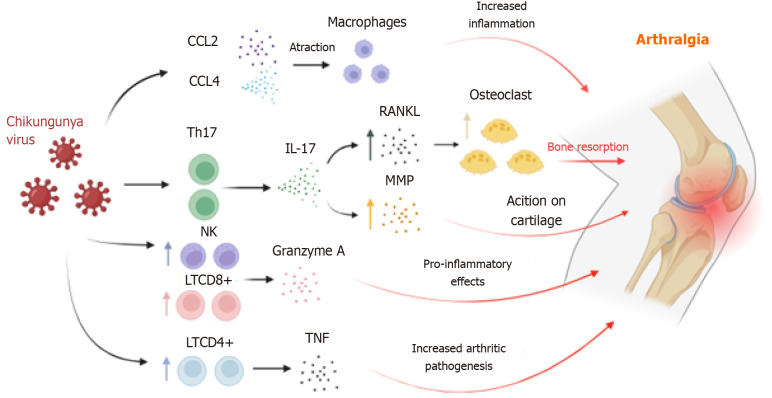
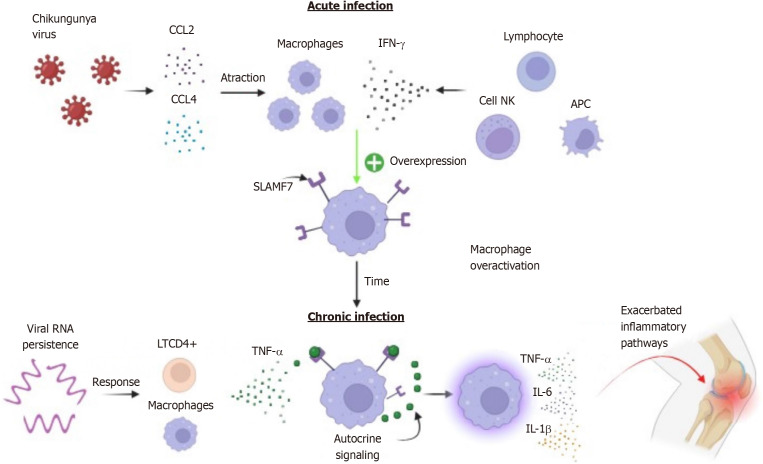
Chikungunya fever (CF) is caused by an arbovirus whose manifestations are extremely diverse, and it has evolved with significant severity in recent years. The clinical signs triggered by the Chikungunya virus are similar to those of other arboviruses. Generally, fever starts abruptly and reaches high levels, followed by severe polyarthralgia and myalgia, as well as an erythematous or petechial maculopapular rash, varying in severity and extent. Around 40% to 60% of affected individuals report persistent arthralgia, which can last from months to years. The symptoms of CF mainly represent the tissue tropism of the virus rather than the immunopathogenesis triggered by the host's immune system. The main mechanisms associated with arthralgia have been linked to an increase in T helper type 17 cells and a consequent increase in receptor activator of nuclear factor kappa-Β ligand and bone resorption. This review suggests that persistent arthralgia results from the presence of viral antigens post-infection and the constant activation of signaling lymphocytic activation molecule family member 7 in synovial macrophages, leading to local infiltration of CD4+ T cells, which sustains the inflammatory process in the joints through the secretion of pro-inflammatory cytokines. The term "long chikungunya" was used in this review to refer to persistent arthralgia since, due to its manifestation over long periods after the end of the viral infection, this clinical condition seems to be characterized more as a sequel than as a symptom, given that there is no active infection involved.
基孔肯雅热(CF)由一种虫媒病毒引起,其表现极为多样,且近年来病情严重程度有所演变。基孔肯雅病毒引发的临床症状与其他虫媒病毒相似。一般来说,发热起病急骤且体温很高,随后出现严重的多关节痛和肌痛,以及红斑或瘀点性斑丘疹,严重程度和范围各不相同。约40%至60%的感染者报告有持续性关节痛,可持续数月至数年。基孔肯雅热的症状主要体现病毒的组织嗜性,而非宿主免疫系统引发的免疫发病机制。与关节痛相关的主要机制与17型辅助性T细胞增多以及随之而来的核因子κB受体激活剂配体增加和骨吸收有关。本综述表明,持续性关节痛是由于感染后病毒抗原的存在以及滑膜巨噬细胞中信号淋巴细胞激活分子家族成员7的持续激活,导致CD4 + T细胞局部浸润,通过分泌促炎细胞因子维持关节内的炎症过程。本综述中使用“长期基孔肯雅病”一词来指代持续性关节痛,因为鉴于病毒感染结束后其症状持续很长时间,这种临床状况似乎更具有后遗症的特征,而非症状,因为此时不存在活跃感染。