Nuffield Department of Primary Care Health Sciences, Bennett Institute for Applied Data Science, Oxford University, Oxford, OX2 6GG, UK.
London School of Hygiene and Tropical Medicine, Keppel Street, London, WC1E 7HT, UK.
BMC Med. 2024 Jul 10;22(1):288. doi: 10.1186/s12916-024-03499-5.
Ethnicity is known to be an important correlate of health outcomes, particularly during the COVID-19 pandemic, where some ethnic groups were shown to be at higher risk of infection and adverse outcomes. The recording of patients' ethnic groups in primary care can support research and efforts to achieve equity in service provision and outcomes; however, the coding of ethnicity is known to present complex challenges. We therefore set out to describe ethnicity coding in detail with a view to supporting the use of this data in a wide range of settings, as part of wider efforts to robustly describe and define methods of using administrative data.
We describe the completeness and consistency of primary care ethnicity recording in the OpenSAFELY-TPP database, containing linked primary care and hospital records in > 25 million patients in England. We also compared the ethnic breakdown in OpenSAFELY-TPP with that of the 2021 UK census.
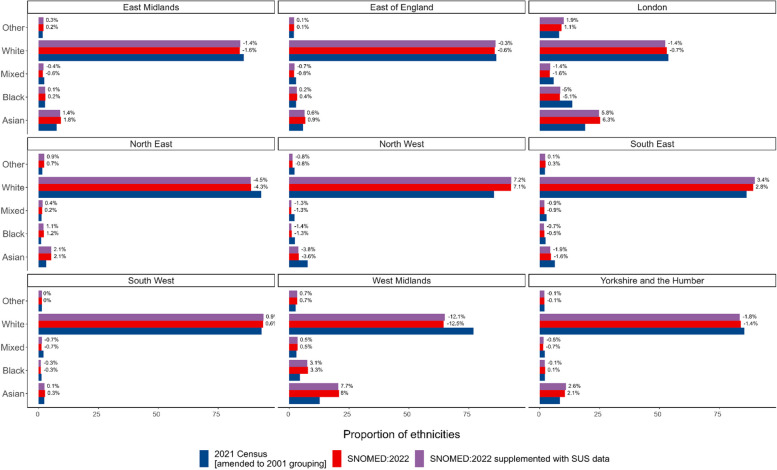
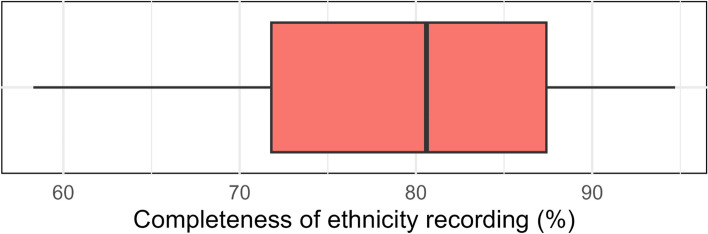
78.2% of patients registered in OpenSAFELY-TPP on 1 January 2022 had their ethnicity recorded in primary care records, rising to 92.5% when supplemented with hospital data. The completeness of ethnicity recording was higher for women than for men. The rate of primary care ethnicity recording ranged from 77% in the South East of England to 82.2% in the West Midlands. Ethnicity recording rates were higher in patients with chronic or other serious health conditions. For each of the five broad ethnicity groups, primary care recorded ethnicity was within 2.9 percentage points of the population rate as recorded in the 2021 Census for England as a whole. For patients with multiple ethnicity records, 98.7% of the latest recorded ethnicities matched the most frequently coded ethnicity. Patients whose latest recorded ethnicity was categorised as Other were most likely to have a discordant ethnicity recording (32.2%).
Primary care ethnicity data in OpenSAFELY is present for over three quarters of all patients, and combined with data from other sources can achieve a high level of completeness. The overall distribution of ethnicities across all English OpenSAFELY-TPP practices was similar to the 2021 Census, with some regional variation. This report identifies the best available codelist for use in OpenSAFELY and similar electronic health record data.
众所周知,种族是健康结果的一个重要相关因素,尤其是在 COVID-19 大流行期间,一些族裔群体被发现感染和不良结果的风险更高。在初级保健中记录患者的种族可以支持研究,并努力实现服务提供和结果的公平;然而,种族的编码已知存在复杂的挑战。因此,我们详细描述了种族编码,以期支持在广泛的环境中使用这些数据,作为更广泛地描述和定义使用行政数据方法的一部分。
我们描述了 OpenSAFELY-TPP 数据库中初级保健种族记录的完整性和一致性,该数据库包含了英格兰 2500 多万患者的链接初级保健和医院记录。我们还将 OpenSAFELY-TPP 中的种族分布与 2021 年英国人口普查进行了比较。
2022 年 1 月 1 日在 OpenSAFELY-TPP 注册的患者中,有 78.2%在初级保健记录中记录了他们的种族,当补充医院数据时,这一比例上升到 92.5%。女性的种族记录完整性高于男性。英格兰东南部的初级保健种族记录率为 77%,西米德兰兹为 82.2%。慢性或其他严重健康状况患者的种族记录率较高。在五个广泛的种族群体中,每个群体的初级保健记录种族与整个英格兰 2021 年人口普查记录的种族比例相差不到 2.9 个百分点。对于有多个种族记录的患者,最新记录的种族中有 98.7%与最常编码的种族相匹配。最新记录的种族被归类为其他的患者最有可能出现种族记录不一致(32.2%)。
OpenSAFELY 中的初级保健种族数据存在于超过四分之三的所有患者中,与其他来源的数据相结合,可以达到高度的完整性。所有英国 OpenSAFELY-TPP 实践中种族的总体分布与 2021 年人口普查相似,存在一些地区差异。本报告确定了在 OpenSAFELY 和类似电子健康记录数据中使用的最佳现有代码列表。