Department of Anesthesiology and Operative Intensive Care Medicine (CCM, CVK), Charité-Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin and Berlin Institute of Health, Campus Virchow-Klinikum, Berlin, Germany.
Institute of Medical Informatics, Charité-Universitätsmedizin Berlin, Berlin, Germany.
PLoS One. 2024 Jul 11;19(7):e0303165. doi: 10.1371/journal.pone.0303165. eCollection 2024.
The outcome of patients undergoing major surgery treated with HES for hemodynamic optimization is unclear. This post-hoc analysis of a randomized clinical pilot trial investigated the impact of low-molecular balanced HES solutions on the coagulation system, blood loss and transfusion requirements.
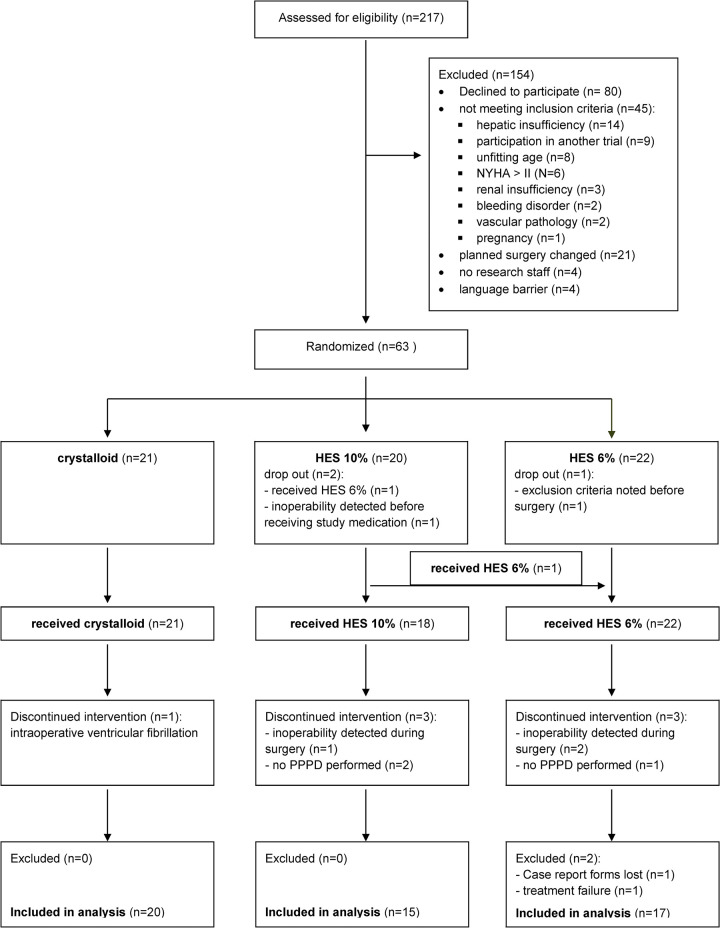
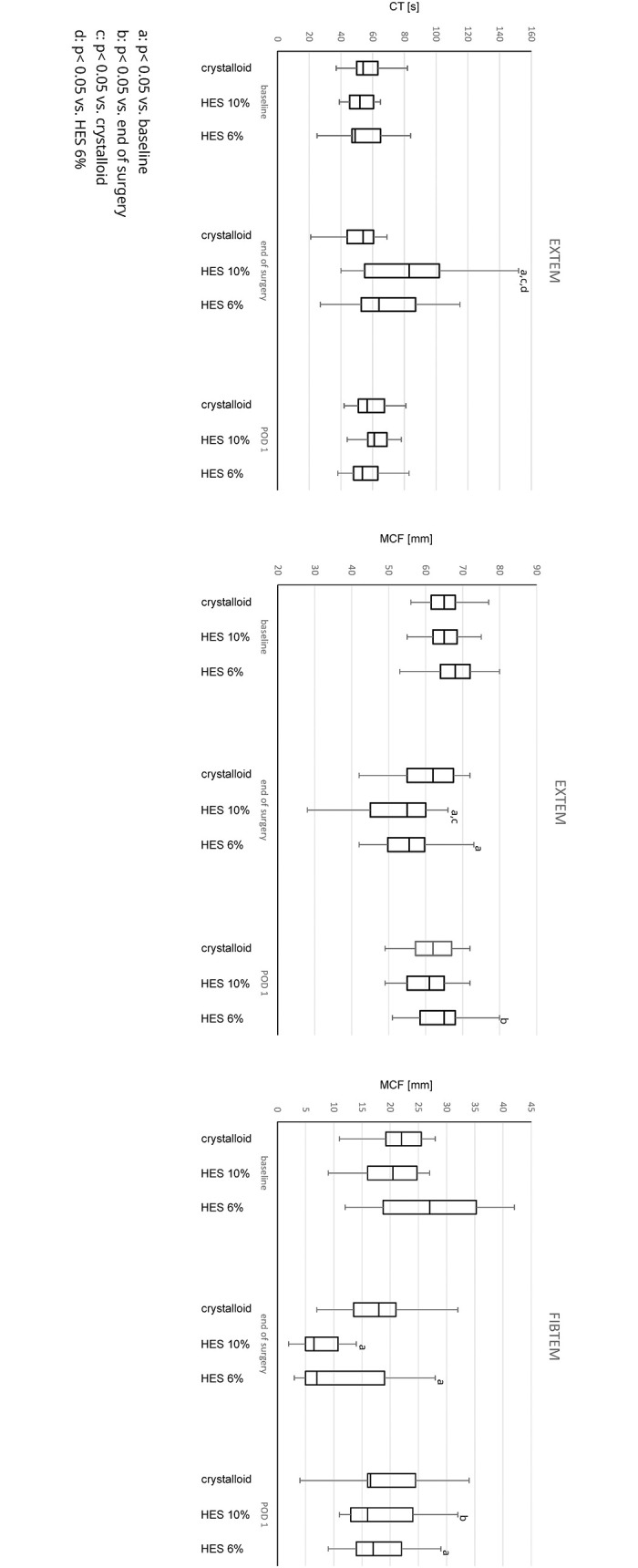
The Trial was registered: EudraCT 2008-004175-22 and ethical approval was provided by the ethics committee of Berlin. Patients were randomized into three groups receiving either a 10% HES 130/0.42 solution, a 6% HES 130/0.42 solution or a crystalloid following a goal-directed hemodynamic algorithm. Endpoints were parameters of standard and viscoelastic coagulation laboratory, blood loss and transfusion requirements at baseline, at the end of surgery (EOS) and the first postoperative day (POD 1).
Fifty-two patients were included in the analysis (HES 10% (n = 15), HES 6% (n = 17) and crystalloid (n = 20)). Fibrinogen decreased in all groups at EOS (HES 10% 338 [298;378] to 192 [163;234] mg dl-1, p<0.01, HES 6% 385 [302;442] to 174 [163;224] mg dl-1, p<0.01, crystalloids 408 [325;458] to 313 [248;370] mg dl-1, p = 0.01). MCF FIBTEM was decreased for both HES groups at EOS (HES 10%: 20.5 [16.0;24.8] to 6.5 [5.0;10.8] mm, p = <0.01; HES 6% 27.0 [18.8;35.2] to 7.0 [5.0;19.0] mm, p = <0.01). These changes did not persist on POD 1 for HES 10% (rise to 16.0 [13.0;24.0] mm, p = 0.88). Blood loss was not different in the groups nor transfusion requirements.
Our data suggest a stronger but transient effect of balanced, low-molecular HES on the coagulation system. Despite the decline of the use of artificial colloids in clinical practice, these results may help to inform clinicians who use HES solutions.
接受 HES 进行血流动力学优化治疗的大手术患者的结局尚不清楚。本研究对一项随机临床试验的事后分析旨在研究低分子平衡 HES 溶液对凝血系统、失血和输血需求的影响。
该试验已在 EudraCT 注册:2008-004175-22,柏林伦理委员会提供了伦理批准。患者随机分为三组,分别接受 10% HES 130/0.42 溶液、6% HES 130/0.42 溶液或晶体液,根据目标导向的血流动力学算法进行治疗。终点为标准和黏弹性凝血实验室参数、基线时、手术结束时(EOS)和术后第 1 天(POD 1)的失血和输血需求。
52 例患者纳入分析(10% HES 组(n = 15)、6% HES 组(n = 17)和晶体液组(n = 20))。EOS 时所有组的纤维蛋白原均降低(10% HES 组:338 [298;378] 至 192 [163;234] mg/dl-1,p<0.01,6% HES 组:385 [302;442] 至 174 [163;224] mg/dl-1,p<0.01,晶体液组:408 [325;458] 至 313 [248;370] mg/dl-1,p = 0.01)。EOS 时,两个 HES 组的 MCF FIBTEM 均降低(HES 10%:20.5 [16.0;24.8] 至 6.5 [5.0;10.8] mm,p<0.01;HES 6%:27.0 [18.8;35.2] 至 7.0 [5.0;19.0] mm,p<0.01)。这些变化在 POD 1 时并未持续存在于 10% HES 组(升高至 16.0 [13.0;24.0] mm,p = 0.88)。各组间失血和输血需求无差异。
我们的数据表明,平衡的低分子 HES 对凝血系统的影响更强但更短暂。尽管胶体在临床实践中的使用有所减少,但这些结果可能有助于告知使用 HES 溶液的临床医生。