Joly Lauren, Virgilio Richard, Yother Claire
Pediatrics, Edward Via College of Osteopathic Medicine, Auburn, USA.
Clinical Affairs, Edward Via College of Osteopathic Medicine, Auburn, USA.
Cureus. 2024 Jun 10;16(6):e62107. doi: 10.7759/cureus.62107. eCollection 2024 Jun.
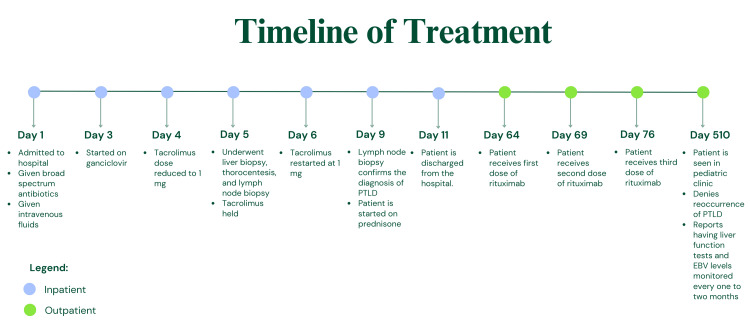
A 13-year-old male with a past medical history of receiving a whole liver transplant secondary to alpha-1 antitrypsin deficiency (AATD) with subsequent inferior vena cava thrombosis nine years prior presented to the emergency department with abdominal distension, shortness of breath, coughing, and left superficial cervical lymphadenopathy. He had seen his pediatrician the day before where he tested negative for group A , influenza, and severe acute respiratory syndrome coronavirus 2. Additionally, the patient reported having elevated liver function tests noted from the results of lab tests taken earlier that day. The patient was admitted to the hospital. While at the hospital, a lymph node biopsy was performed, and pathology from that biopsy revealed infectious mononucleosis-like nondestructive posttransplant lymphoproliferative disorder (PTLD). Due to the patient's liver transplant nine years prior, the patient was on an immunosuppressant medication: tacrolimus 2 mg. To treat the PTLD, the tacrolimus was reduced, then stopped, and then subsequently restarted at 1 mg. He also was given ganciclovir and prednisone. Two months after recovering from the PTLD, the patient's Epstein-Barr-virus (EBV) viral load continued to fluctuate, and he was treated with three doses of the monoclonal antibody drug rituximab. After treatment with rituximab, his EBV viral load remained stable. This case report gives insight into the treatment of PTLD and can serve as a reminder to be aware of the possibility of PTLD in a pediatric patient with AATD multiple years after a transplant.
一名13岁男性,既往有因α-1抗胰蛋白酶缺乏症(AATD)接受全肝移植的病史,9年前出现下腔静脉血栓形成,现因腹胀、呼吸急促、咳嗽和左颈浅淋巴结肿大就诊于急诊科。前一天他看过儿科医生,甲型流感和严重急性呼吸综合征冠状病毒2检测均为阴性。此外,患者报告当天早些时候的实验室检查结果显示肝功能检查结果升高。患者被收入院。在医院期间,进行了淋巴结活检,活检病理显示为传染性单核细胞增多症样非破坏性移植后淋巴细胞增生性疾病(PTLD)。由于患者9年前接受了肝移植,正在服用免疫抑制剂他克莫司2毫克。为治疗PTLD,他克莫司剂量先减少,然后停用,随后又以1毫克重新开始服用。他还接受了更昔洛韦和泼尼松治疗。从PTLD恢复两个月后,患者的爱泼斯坦-巴尔病毒(EBV)病毒载量持续波动,他接受了三剂单克隆抗体药物利妥昔单抗治疗。使用利妥昔单抗治疗后,他的EBV病毒载量保持稳定。本病例报告深入探讨了PTLD的治疗方法,并提醒人们注意移植多年后患有AATD的儿科患者发生PTLD的可能性。