Yang Zhou Jordi, Eder Dominik, Weber Florian, Heumann Philipp, Kronenberg Katharina, Werner Jens M, Geissler Edward K, Schlitt Hans J, Hutchinson James A, Bitterer Florian
Department of Surgery, University Hospital Regensburg, Regensburg, Germany.
Leibniz Institute for Immunotherapy, University Hospital Regensburg, Regensburg, Germany.
Front Transplant. 2023 Aug 14;2:1211916. doi: 10.3389/frtra.2023.1211916. eCollection 2023.
The approval of Atezolizumab / Bevacizumab therapy (Atezo/Bev) in 2020 opened up a promising new treatment option for patients with end-stage hepatocellular carcinoma (HCC). However, liver transplant (LTx) patients with HCC are still denied this therapy owing to concerns about ICI-induced organ rejection and lack of regulatory approval.
A prospective observational study at a tertiary liver transplant centre monitored the compassionate, off-label use of Atezo/Bev in a single, stable LTx recipient with non-resectable HCC recurrence. Close clinical, laboratory and immunological monitoring of the patient was performed throughout a four-cycle Atezo/Bev treatment. Measured parameters were selected after a systematic review of the literature on predictive markers for clinical response and risk of graft rejection caused by ICI therapy.
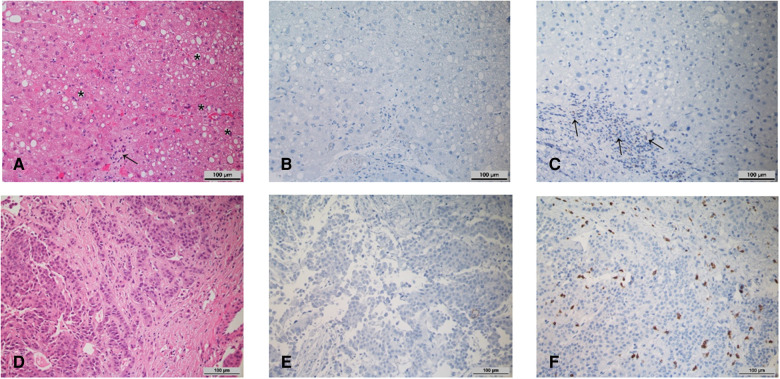
19 articles describing 20 unique predictive biomarkers were identified. The most promising negative prognostic factors were the baseline values and dynamic course of IL-6, alpha-fetoprotein (AFP) and the AFP/CRP ratio. The frequency of regulatory T cells (Treg) reportedly correlates with the success of ICI therapy. PD-L1 and CD28 expression level with the allograft, peripheral blood CD4 T cell numbers and Torque Teno Virus (TTV) titre may predict risk of LTx rejection following ICI therapy. No relevant side effects or acute rejection occurred during Atezo/Bev therapy; however, treatment did not prevent tumor progression. Absence of PD-L1 expression in pre-treatment liver biopsies, as well as a progressive downregulation of CD28 expression by CD4 T cells during therapy, correctly predicted absence of rejection. Furthermore, increased IL-6 and AFP levels after starting therapy, as well as a reduction in blood Treg frequency, correctly anticipated a lack of therapeutic response.
Atezo/Bev therapy for unresectable HCC in stable LTx patients remains a controversial strategy because it carries a high-risk of rejection and therapeutic response rates are poorly defined. Although previously described biomarkers of rejection risk and therapeutic response agreed with clinical outcomes in the described case, these immunological parameters are difficult to reliably interpret. Clearly, there is an important unmet need for standardized assays and clinically validated cut-offs before we use these biomarkers to guide treatment decisions for our patients.
2020年阿替利珠单抗/贝伐珠单抗疗法(阿替利珠单抗/贝伐单抗,Atezo/Bev)获批,为晚期肝细胞癌(HCC)患者开辟了一种前景广阔的新治疗选择。然而,由于担心免疫检查点抑制剂(ICI)引起的器官排斥反应以及缺乏监管批准,肝癌肝移植(LTx)患者仍无法接受这种治疗。
在一家三级肝移植中心进行的一项前瞻性观察性研究,监测了阿替利珠单抗/贝伐单抗在一名患有不可切除肝癌复发的稳定肝移植受者中的同情性、超适应症使用情况。在整个四个周期的阿替利珠单抗/贝伐单抗治疗过程中,对患者进行了密切的临床、实验室和免疫学监测。在系统回顾关于ICI治疗临床反应和移植排斥风险预测标志物的文献后,选择了测量参数。
共鉴定出19篇描述20种独特预测生物标志物的文章。最有希望的负面预后因素是白细胞介素-6(IL-6)、甲胎蛋白(AFP)的基线值和动态变化过程以及AFP/CRP比值。据报道,调节性T细胞(Treg)的频率与ICI治疗的成功率相关。移植器官的程序性死亡受体1(PD-L1)和CD28表达水平、外周血CD4 T细胞数量以及Torque Teno病毒(TTV)滴度可能预测ICI治疗后肝移植排斥反应的风险。在阿替利珠单抗/贝伐单抗治疗期间未发生相关副作用或急性排斥反应;然而,治疗并未阻止肿瘤进展。治疗前肝活检中PD-L1表达缺失,以及治疗期间CD4 T细胞对CD28表达的逐渐下调,正确预测了无排斥反应。此外,治疗开始后IL-6和AFP水平升高,以及血液中Treg频率降低,正确预测了缺乏治疗反应。
在稳定的肝移植患者中,阿替利珠单抗/贝伐单抗治疗不可切除肝癌仍然是一种有争议的策略,因为它有很高的排斥风险,且治疗反应率尚不明确。尽管先前描述的排斥风险和治疗反应生物标志物与所述病例的临床结果一致,但这些免疫参数难以可靠地解释。显然,在我们使用这些生物标志物来指导患者的治疗决策之前,迫切需要标准化检测方法和经过临床验证的临界值。