Ballin Marcel, Berglind Daniel, Henriksson Pontus, Neovius Martin, Nordström Anna, Ortega Francisco B, Sillanpää Elina, Nordström Peter, Ahlqvist Viktor H
Department of Public Health and Caring Sciences, Clinical Geriatrics, Uppsala University, Uppsala, Sweden.
Centre for Epidemiology and Community Medicine, Region Stockholm, Stockholm, Sweden.
medRxiv. 2024 Jul 3:2024.07.01.24309761. doi: 10.1101/2024.07.01.24309761.
To investigate whether the higher risks of certain cancers associated with high cardiorespiratory fitness can be explained by increased detection and unobserved confounders.
Nationwide sibling-controlled cohort study of adolescents.
Sweden.
1 124 049 men of which 477 453 were full siblings, who underwent mandatory military conscription examinations between 1972 and 1995 at a mean age of 18.3 years.
Hazard ratios (HR) and 95% confidence intervals (CI) of overall cancer diagnosis and cancer mortality, and 14 site-specific cancers (diagnosis or death), as recorded in the Swedish National Patient Register or Cause of Death Register until 31 December 2023, modelled using flexible parametric regressions.
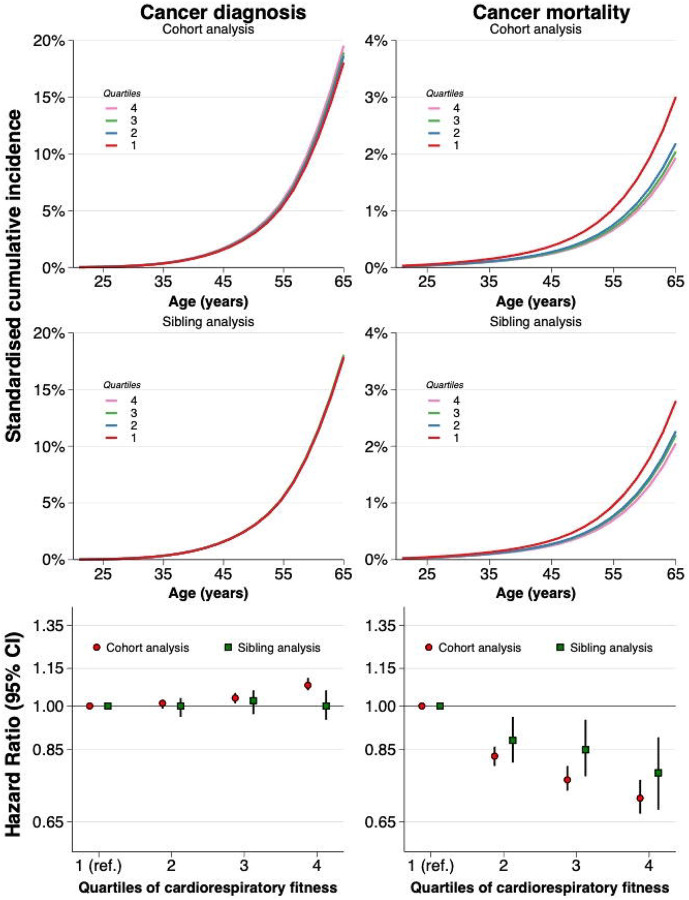
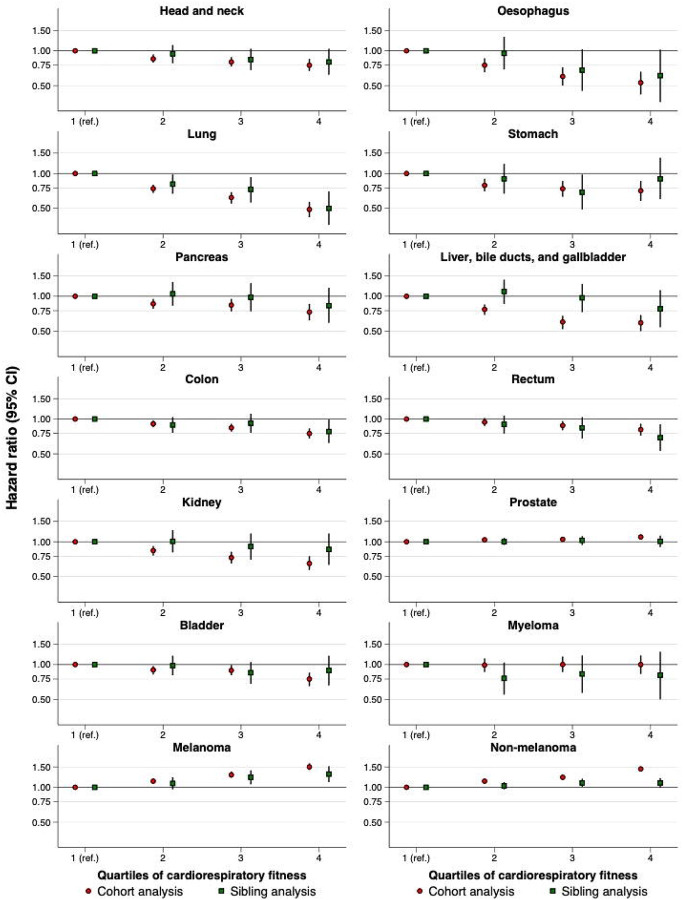
Participants were followed until a median (maximum) age of 55.9 (73.5) years, during which 98 410 were diagnosed with cancer and 16 789 had a cancer-related death (41 293 and 6908 among full siblings respectively). The most common cancers were non-melanoma skin (27 105 diagnoses & 227 deaths) and prostate cancer (24 211 diagnoses & 869 deaths). In cohort analysis, those in the highest quartile of cardiorespiratory fitness had a higher risk of prostate (adjusted HR 1.10; 95% CI: 1.05 to 1.16) and skin cancer (e.g., non-melanoma HR 1.44; 1.37 to 1.50) compared to those in the lowest quartile, which led to a higher risk of any type of cancer diagnosis (HR 1.08; 1.06 to 1.11). However, those in the highest quartile had a lower risk of cancer mortality (HR 0.71; 0.67 to 0.76). When comparing full siblings, and thereby controlling for all behavioural, environmental, and genetic factors they share, the excess risk of prostate (HR 1.01; 0.90 to 1.13) and skin cancer (e.g., non-melanoma HR 1.09; 0.99 to 1.20) attenuated to the null. In contrast, the lower risk of overall cancer mortality was still statistically significant after control for such shared confounders (HR 0.78; 0.68 to 0.89). For other site-specific cancers, the influence of such confounding tended to vary, but none showed the same excess risk as prostate and non-melanoma skin cancer.
The association between high levels of adolescent cardiorespiratory fitness and excess risk of some cancers, such as prostate and non-melanoma skin cancer, appears to be fully explained by unobserved confounders shared between full siblings. However, the protective association with cancer mortality persists even after control for such confounding.
探讨与高心肺适能相关的某些癌症风险增加是否可通过检测增加和未观察到的混杂因素来解释。
全国范围内对青少年进行的同胞对照队列研究。
瑞典。
1124049名男性,其中477453名是同胞兄弟,他们于1972年至1995年间平均年龄18.3岁时接受了义务兵役检查。
截至2023年12月31日,瑞典国家患者登记册或死亡原因登记册记录的总体癌症诊断和癌症死亡率以及14种特定部位癌症(诊断或死亡)的风险比(HR)和95%置信区间(CI),采用灵活参数回归模型进行建模。
参与者随访至中位(最大)年龄55.9(73.5)岁,在此期间,98410人被诊断患有癌症,16789人死于癌症相关疾病(同胞兄弟中分别为41293人和6908人)。最常见的癌症是非黑色素瘤皮肤癌(27105例诊断和227例死亡)和前列腺癌(24211例诊断和869例死亡)。在队列分析中,与心肺适能最低四分位数的人相比,心肺适能最高四分位数的人患前列腺癌(调整后HR 1.10;95%CI:1.05至1.16)和皮肤癌(如非黑色素瘤HR 1.44;1.37至1.50)的风险更高,这导致任何类型癌症诊断的风险更高(HR 1.08;1.06至1.11)。然而,最高四分位数的人癌症死亡率风险较低(HR 0.71;0.67至0.76)。在比较同胞兄弟并控制他们共有的所有行为、环境和遗传因素时,前列腺癌(HR 1.01;0.90至1.13)和皮肤癌(如非黑色素瘤HR 1.09;0.99至1.20)的额外风险减弱至零。相比之下,在控制了这些共同的混杂因素后,总体癌症死亡率较低的风险仍然具有统计学意义(HR 0.78;0.68至0.89)。对于其他特定部位癌症,这种混杂因素的影响往往有所不同,但没有一种显示出与前列腺癌和非黑色素瘤皮肤癌相同的额外风险。
青少年高水平心肺适能与某些癌症(如前列腺癌和非黑色素瘤皮肤癌)的额外风险之间的关联似乎完全可以由同胞兄弟共有的未观察到的混杂因素来解释。然而,即使在控制了这种混杂因素之后,与癌症死亡率的保护关联仍然存在。