Biostatistics Support and Research Unit, Germans Trias I Pujol Research Institute and Hospital (IGTP), Campus Can RutiCarretera de Can RutiCamí de Les Escoles S/N, Barcelona, Badalona, 08916, Spain.
Department of Basic Clinical Practice, School of Medicine and Health Sciences, University of Barcelona, Barcelona, Spain.
BMC Palliat Care. 2024 Jul 16;23(1):173. doi: 10.1186/s12904-024-01490-8.
Therapeutic ceiling of care is the maximum level of care deemed appropiate to offer to a patient based on their clinical profile and therefore their potential to derive benefit, within the context of the availability of resources. To our knowledge, there are no models to predict ceiling of care decisions in COVID-19 patients or other acute illnesses. We aimed to develop and validate a clinical prediction model to predict ceiling of care decisions using information readily available at the point of hospital admission.
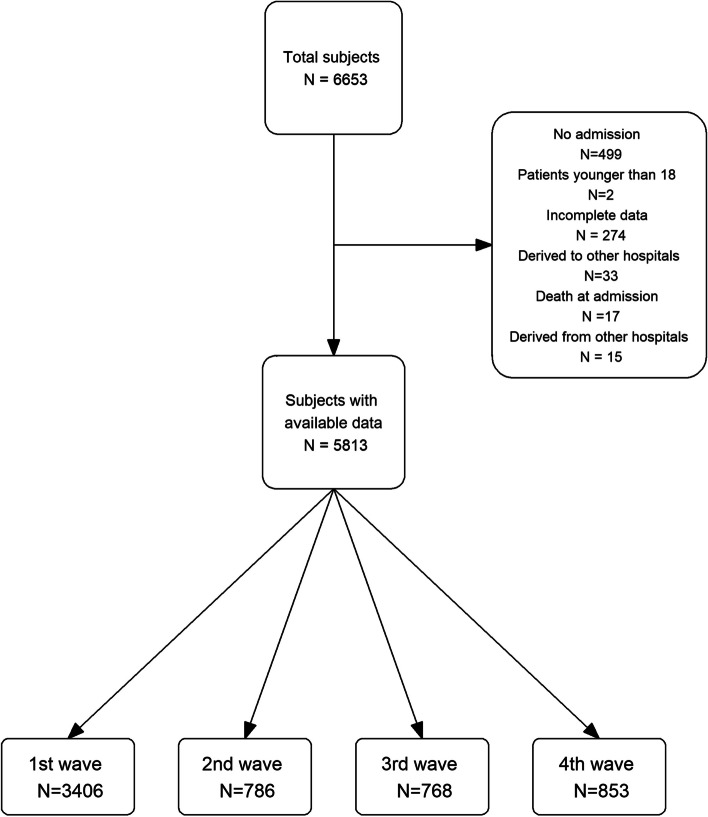
We studied a cohort of adult COVID-19 patients who were hospitalized in 5 centres of Catalonia between 2020 and 2021. All patients had microbiologically proven SARS-CoV-2 infection at the time of hospitalization. Their therapeutic ceiling of care was assessed at hospital admission. Comorbidities collected at hospital admission, age and sex were considered as potential factors for predicting ceiling of care. A logistic regression model was used to predict the ceiling of care. The final model was validated internally and externally using a cohort obtained from the Leeds Teaching Hospitals NHS Trust. The TRIPOD Checklist for Prediction Model Development and Validation from the EQUATOR Network has been followed to report the model.
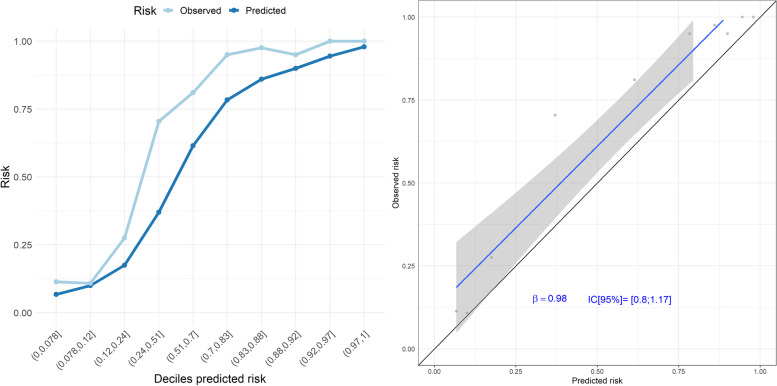
A total of 5813 patients were included in the development cohort, of whom 31.5% were assigned a ceiling of care at the point of hospital admission. A model including age, COVID-19 wave, chronic kidney disease, dementia, dyslipidaemia, heart failure, metastasis, peripheral vascular disease, chronic obstructive pulmonary disease, and stroke or transient ischaemic attack had excellent discrimination and calibration. Subgroup analysis by sex, age group, and relevant comorbidities showed excellent figures for calibration and discrimination. External validation on the Leeds Teaching Hospitals cohort also showed good performance.
Ceiling of care can be predicted with great accuracy from a patient's clinical information available at the point of hospital admission. Cohorts without information on ceiling of care could use our model to estimate the probability of ceiling of care. In future pandemics, during emergency situations or when dealing with frail patients, where time-sensitive decisions about the use of life-prolonging treatments are required, this model, combined with clinical expertise, could be valuable. However, future work is needed to evaluate the use of this prediction tool outside COVID-19.
治疗护理上限是指根据患者的临床特征和受益潜力,在资源可及的情况下,认为最适合为患者提供的护理水平。据我们所知,目前还没有针对 COVID-19 患者或其他急性疾病的护理上限决策预测模型。我们旨在开发和验证一种临床预测模型,使用入院时即可获得的信息来预测护理上限决策。
我们研究了一组 2020 年至 2021 年期间在加泰罗尼亚 5 家中心住院的成年 COVID-19 患者。所有患者在入院时均被证实存在 SARS-CoV-2 感染。他们的治疗护理上限在入院时进行评估。入院时收集的合并症、年龄和性别被视为预测护理上限的潜在因素。使用逻辑回归模型预测护理上限。最终模型在内部和外部使用来自利兹教学医院 NHS 信托基金的队列进行验证。该模型遵循了 EQUATOR 网络的预测模型开发和验证的 TRIPOD 清单进行报告。
共有 5813 例患者纳入开发队列,其中 31.5%的患者在入院时被分配了护理上限。一个包含年龄、COVID-19 波次、慢性肾脏病、痴呆、血脂异常、心力衰竭、转移、外周血管疾病、慢性阻塞性肺疾病以及中风或短暂性脑缺血发作的模型具有出色的区分度和校准度。按性别、年龄组和相关合并症进行的亚组分析显示了出色的校准和区分度。在利兹教学医院队列的外部验证也显示了良好的性能。
从患者入院时的临床信息中,可以非常准确地预测护理上限。没有护理上限信息的队列可以使用我们的模型来估计护理上限的概率。在未来的大流行中,在紧急情况下或处理脆弱患者时,需要对延长生命的治疗的使用做出时间敏感的决策,该模型结合临床专业知识,可能具有价值。然而,未来需要评估该预测工具在 COVID-19 之外的使用。