Department of Radiological Sciences, University of California, Irvine, California, United States of America.
Department of Radiological Sciences, Emory University, Atlanta, Georgia, United States of America.
PLoS One. 2020 Dec 9;15(12):e0242953. doi: 10.1371/journal.pone.0242953. eCollection 2020.
The rapid spread of coronavirus disease 2019 (COVID-19) revealed significant constraints in critical care capacity. In anticipation of subsequent waves, reliable prediction of disease severity is essential for critical care capacity management and may enable earlier targeted interventions to improve patient outcomes. The purpose of this study is to develop and externally validate a prognostic model/clinical tool for predicting COVID-19 critical disease at presentation to medical care.
This is a retrospective study of a prognostic model for the prediction of COVID-19 critical disease where critical disease was defined as ICU admission, ventilation, and/or death. The derivation cohort was used to develop a multivariable logistic regression model. Covariates included patient comorbidities, presenting vital signs, and laboratory values. Model performance was assessed on the validation cohort by concordance statistics. The model was developed with consecutive patients with COVID-19 who presented to University of California Irvine Medical Center in Orange County, California. External validation was performed with a random sample of patients with COVID-19 at Emory Healthcare in Atlanta, Georgia.
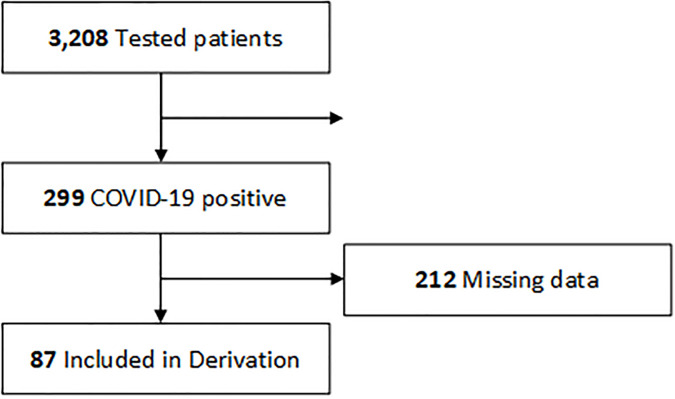
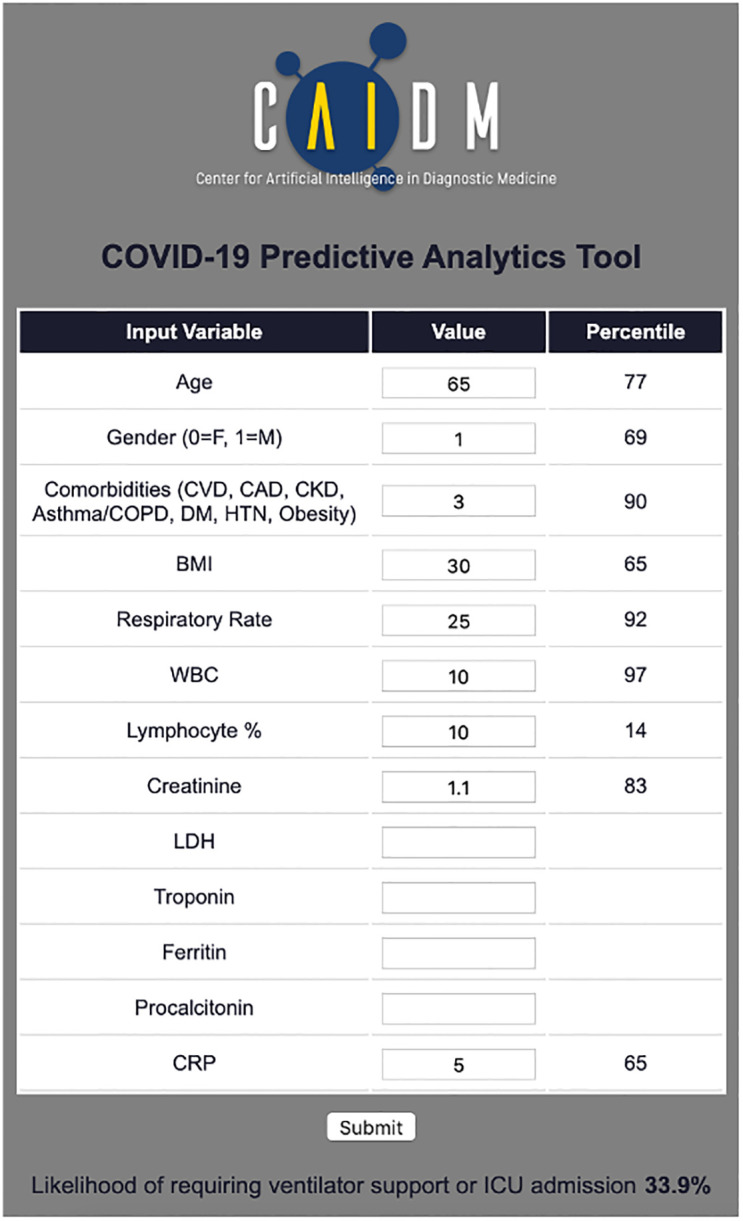
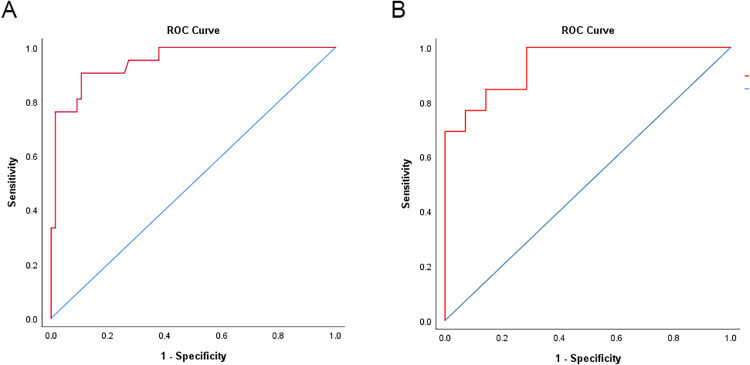
Of a total 3208 patients tested in the derivation cohort, 9% (299/3028) were positive for COVID-19. Clinical data including past medical history and presenting laboratory values were available for 29% (87/299) of patients (median age, 48 years [range, 21-88 years]; 64% [36/55] male). The most common comorbidities included obesity (37%, 31/87), hypertension (37%, 32/87), and diabetes (24%, 24/87). Critical disease was present in 24% (21/87). After backward stepwise selection, the following factors were associated with greatest increased risk of critical disease: number of comorbidities, body mass index, respiratory rate, white blood cell count, % lymphocytes, serum creatinine, lactate dehydrogenase, high sensitivity troponin I, ferritin, procalcitonin, and C-reactive protein. Of a total of 40 patients in the validation cohort (median age, 60 years [range, 27-88 years]; 55% [22/40] male), critical disease was present in 65% (26/40). Model discrimination in the validation cohort was high (concordance statistic: 0.94, 95% confidence interval 0.87-1.01). A web-based tool was developed to enable clinicians to input patient data and view likelihood of critical disease.
We present a model which accurately predicted COVID-19 critical disease risk using comorbidities and presenting vital signs and laboratory values, on derivation and validation cohorts from two different institutions. If further validated on additional cohorts of patients, this model/clinical tool may provide useful prognostication of critical care needs.
新冠病毒疾病 2019(COVID-19)的迅速传播显示出重症监护能力的重大限制。为了应对后续的浪潮,对疾病严重程度的可靠预测对于重症监护能力的管理至关重要,并且可能使更早的有针对性的干预措施得以改善患者的预后。本研究的目的是开发和外部验证一种用于预测 COVID-19 患者在医疗保健就诊时出现重症疾病的预测模型/临床工具。
这是一项针对 COVID-19 重症疾病预测的预后模型的回顾性研究,其中重症疾病定义为 ICU 入院、通气和/或死亡。推导队列用于开发多变量逻辑回归模型。协变量包括患者合并症、就诊时的生命体征和实验室值。在验证队列中通过一致性统计数据评估模型性能。该模型是使用加利福尼亚州奥兰治县加利福尼亚大学欧文医疗中心就诊的连续 COVID-19 患者开发的。在佐治亚州亚特兰大的埃默里医疗保健中心对 COVID-19 患者进行了随机抽样进行外部验证。
在推导队列的 3208 名接受检测的患者中,9%(299/3028)的 COVID-19 检测呈阳性。可获得 29%(87/299)患者的临床数据,包括既往病史和就诊时的实验室值(中位数年龄为 48 岁[范围为 21-88 岁];64%[36/55]为男性)。最常见的合并症包括肥胖症(37%,31/87)、高血压(37%,32/87)和糖尿病(24%,24/87)。重症疾病发生率为 24%(21/87)。经过逐步向后选择,与重症疾病风险增加最大相关的因素如下:合并症数量、体重指数、呼吸频率、白细胞计数、%淋巴细胞、血清肌酐、乳酸脱氢酶、高敏肌钙蛋白 I、铁蛋白、降钙素原和 C 反应蛋白。在验证队列的 40 名患者中(中位数年龄为 60 岁[范围为 27-88 岁];55%[22/40]为男性),65%(26/40)出现重症疾病。验证队列中的模型区分度较高(一致性统计量:0.94,95%置信区间 0.87-1.01)。开发了一个基于网络的工具,使临床医生能够输入患者数据并查看重症疾病的可能性。
我们提出了一种模型,该模型使用合并症和就诊时的生命体征和实验室值,在来自两个不同机构的推导和验证队列中准确预测了 COVID-19 重症疾病的风险。如果在更多的患者队列中进一步验证,该模型/临床工具可能有助于对重症监护需求进行预后预测。