Nusshag Christian, Theobald Vivienne, Wortmann Markus, Kaimann Philipp, Dietrich Maximilian, Gruneberg Daniel, Tourelle Kevin, von der Forst Maik, Weigand Markus A, Bischoff Moritz S, Böckler Dittmar, Schmitt Felix C F
Department of Nephrology, Medical Faculty Heidelberg, Heidelberg University, Heidelberg, Germany.
Department of Anesthesiology, Medical Faculty Heidelberg, Heidelberg University, Heidelberg, Germany.
Front Med (Lausanne). 2024 Jul 3;11:1386018. doi: 10.3389/fmed.2024.1386018. eCollection 2024.
Acute kidney injury (AKI) is a common complication in patients undergoing major vascular surgery. Despite significant research efforts in this area, the incidence of AKI remains high, posing a significant challenge to healthcare systems, especially in situations where resources are limited. Early prediction of AKI severity and individualized postoperative care is therefore essential.
The primary objective of this exploratory study was to assess the diagnostic value of urine cell-cycle arrest biomarkers [(TIMP-2) × (IGFBP7)] and soluble urokinase plasminogen activator receptor (suPAR) for predicting moderate or severe AKI within 24 h after open aortic surgery, and compared to routine kidney biomarkers. Seventy-five patients undergoing elective aortic surgery were included. Clinical parameters, urine and blood samples were collected preoperatively, immediately postoperatively, and 24 h later. AKI was defined using KDIGO criteria. Individual and combined diagnostic performance of biomarkers were evaluated.
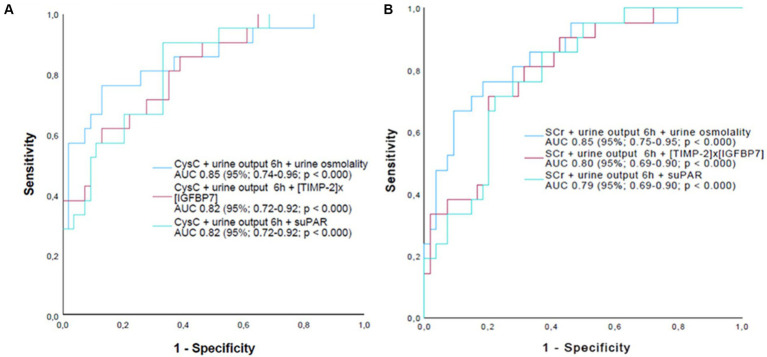
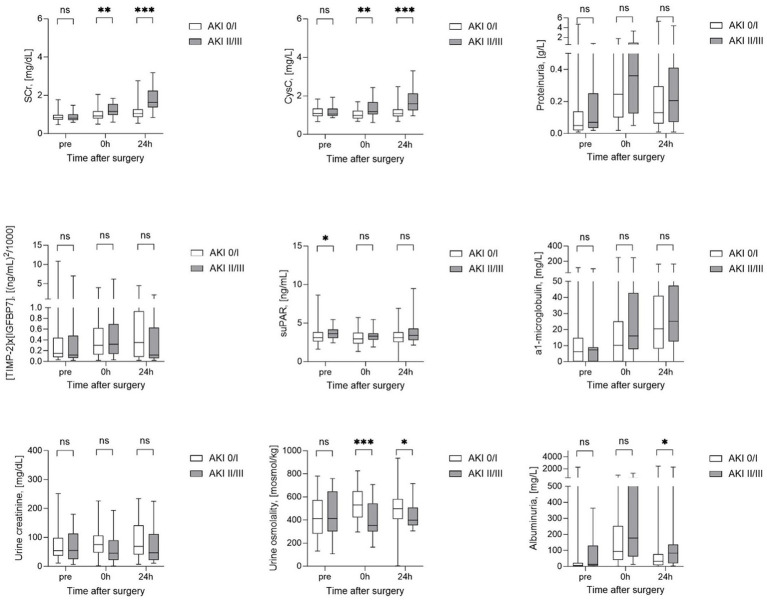
Of the 75 patients, 61% developed AKI, of which 28% developed moderate or severe AKI within 24 h of surgery. Baseline demographics, comorbidities and kidney parameters did not differ between patients with moderate or severe AKI (AKI II/III) and none or mild AKI (AKI 0/I), except for higher preoperative suPAR levels in later AKI II/III patients. Urine osmolality, Cystatin C and serum creatinine had the highest predictive power for AKI II/III with AUCs of 0.75-0.72. (TIMP-2) × (IGFBP7), and neither (TIMP-2) × (IGFBP7) nor suPAR individually showed superior diagnostic value. Combining CysC or SCr with urine osmolality and 6 h urine output gave the best performance with AUCs of 0.86 (95% CI, 0.74-0.96) and 0.85 (95% CI, 0.75-0.95) respectively.
Our study suggests that routine parameters like urine osmolality, CysC, SCr and 6 h urine output perform best in predicting postoperative AKI after aortic surgery compared to the new biomarkers (TIMP-2) × (IGFBP7) and suPAR. Combining biomarkers, particularly CysC or SCr with urine output, urine osmolality, may enhance diagnostic accuracy. Further validation in larger cohorts and clinical settings is warranted to establish their clinical utility.
急性肾损伤(AKI)是接受大血管手术患者的常见并发症。尽管该领域已开展大量研究工作,但AKI的发病率仍然很高,这给医疗系统带来了重大挑战,尤其是在资源有限的情况下。因此,早期预测AKI严重程度并进行个体化术后护理至关重要。
本探索性研究的主要目的是评估尿细胞周期停滞生物标志物[(TIMP-2)×(IGFBP7)]和可溶性尿激酶型纤溶酶原激活物受体(suPAR)对开放主动脉手术后24小时内中度或重度AKI的诊断价值,并与常规肾脏生物标志物进行比较。纳入75例接受择期主动脉手术的患者。术前、术后即刻和术后24小时收集临床参数、尿液和血液样本。根据KDIGO标准定义AKI。评估生物标志物的个体和联合诊断性能。
75例患者中,61%发生AKI,其中28%在手术24小时内发生中度或重度AKI。中度或重度AKI(AKI II/III)患者与无AKI或轻度AKI(AKI 0/I)患者的基线人口统计学、合并症和肾脏参数无差异,但AKI II/III期患者术前suPAR水平较高。尿渗透压、胱抑素C和血清肌酐对AKI II/III的预测能力最强,AUC为0.75 - 0.72。(TIMP-2)×(IGFBP7),以及(TIMP-2)×(IGFBP7)和suPAR单独均未显示出优越的诊断价值。将胱抑素C或血清肌酐与尿渗透压和6小时尿量相结合表现最佳,AUC分别为0.86(95%CI,0.74 - 0.96)和0.85(95%CI,0.75 - 0.95)。
我们的研究表明,与新的生物标志物(TIMP-2)×(IGFBP7)和suPAR相比,尿渗透压、胱抑素C、血清肌酐和6小时尿量等常规参数在预测主动脉手术后的术后AKI方面表现最佳。联合生物标志物,特别是胱抑素C或血清肌酐与尿量、尿渗透压,可能会提高诊断准确性。有必要在更大的队列和临床环境中进行进一步验证,以确定它们的临床实用性。