Department of Neurology, Center for Brain and Mind Health, Yale University School of Medicine, New Haven, Connecticut.
Department of Internal Medicine, Yale University School of Medicine, New Haven, Connecticut.
JAMA Netw Open. 2024 Jul 1;7(7):e2423677. doi: 10.1001/jamanetworkopen.2024.23677.
Stroke secondary prevention trials have disproportionately enrolled participants with mild or no disability. The impact of this bias remains unclear.
To investigate the association between poststroke disability and the rate of recurrent stroke during long-term follow up.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study is a post hoc analysis of the Prevention Regimen For Effectively Avoiding Second Strokes (PRoFESS) and Insulin Resistance Intervention After Stroke (IRIS) secondary prevention clinical trial datasets. PRoFESS enrolled patients from 2003 to 2008, and IRIS enrolled patients from 2005 to 2015. Data were analyzed from September 23, 2023, to May 16, 2024.
The exposure was poststroke functional status at study baseline, defined as modified Rankin Scale (mRS; range, 0-5; higher score indicates more disability) score of 0 vs 1 to 2 vs 3 or greater.
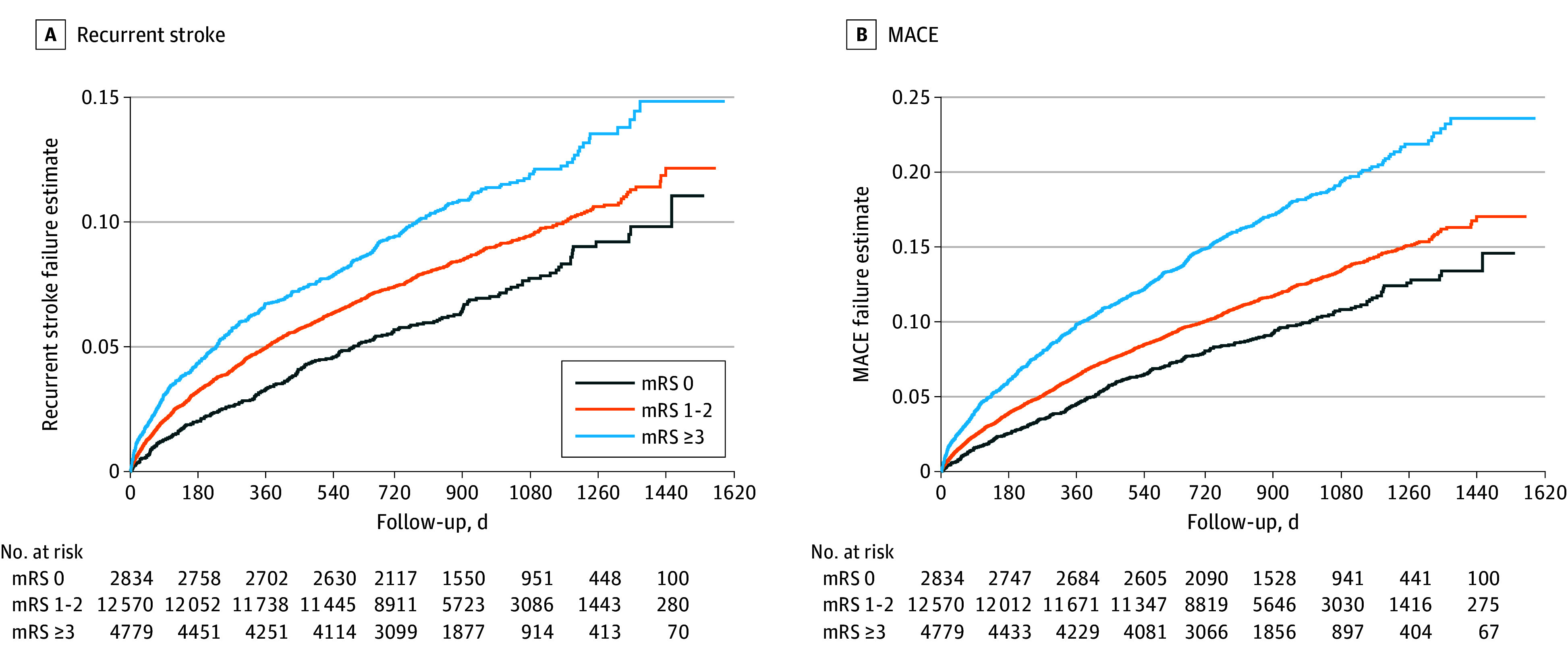
The primary outcome was recurrent stroke. The secondary outcome was major cardiovascular events (MACE), defined as recurrent stroke, myocardial infarction, new or worsening heart failure, or vascular death.
A total of 20 183 PRoFESS participants (mean [SD] age, 66.1 [8.5] years; 12 931 [64.1%] male) and 3265 IRIS participants (mean [SD] age, 62.7 [10.6] years; 2151 [65.9%] male) were included. The median (IQR) follow-up was 2.4 (1.9-3.0) years in PRoFESS and 4.7 (3.2-5.0) years in IRIS. In PRoFESS, the recurrent stroke rate was 7.2%, among patients with an mRS of 0, 8.7% among patients with an mRS of 1 or 2, and 10.6% among patients with an mRS of 3 or greater (χ22 = 27.1; P < .001); in IRIS the recurrent stroke rate was 6.4% among patients with an mRS of 0, 9.0% among patients with an mRS of 1 or 2, and 11.7% among patients with an mRS of 3 or greater (χ22 = 11.1; P < .001). The MACE rate was 10.1% among patients with an mRS of 0, 12.2% among patients with an mRS of 1 or 2, and 17.2% among patients with an mRS of 3 or greater (χ22 = 103.4; P < .001) in PRoFESS and 10.9% among patients with an mRS of 0, 13.3% among patients with an mRS of 1 or 2, and 15.3% among patients with an mRS of 3 or greater (χ22 = 5.8; P = .06) in IRIS. Compared with patients with an mRS of 0, patients with an mRS of 3 or greater had increased hazard for recurrent stroke in PRoFESS (hazard ratio [HR], 1.63; 95% CI, 1.38-1.92; P < .001) and in IRIS (HR, 1.91; 95% CI, 1.28-2.86; P = .002). There was also increased hazard for MACE in PRoFESS (HR, 1.90; 95% CI, 1.66-2.18; P < .001) and in IRIS (HR, 1.45; 95% CI, 1.03-2.03; P = .03).
This cohort study found that higher baseline poststroke disability was associated with increased rates of recurrent stroke and MACE. Including more patients with greater baseline disability in stroke prevention trials may improve the statistical power and generalizability of these studies.
中风二级预防试验不成比例地纳入了轻度或无残疾的参与者。这种偏见的影响仍不清楚。
研究中风后残疾与长期随访期间复发性中风的发生率之间的关系。
设计、地点和参与者:本队列研究是预防有效避免第二次中风(PRoFESS)和中风后胰岛素抵抗干预(IRIS)二级预防临床试验数据集的事后分析。PRoFESS 于 2003 年至 2008 年招募患者,IRIS 于 2005 年至 2015 年招募患者。数据于 2023 年 9 月 23 日至 2024 年 5 月 16 日进行分析。
研究基础上的中风后功能状态为暴露因素,定义为改良 Rankin 量表(mRS;范围为 0-5;得分越高表示残疾程度越高)评分 0 与 1-2 与 3 或更高。
主要结局是复发性中风。次要结局是主要心血管事件(MACE),定义为复发性中风、心肌梗死、新出现或恶化的心力衰竭或血管性死亡。
共纳入 20183 名 PRoFESS 参与者(平均[标准差]年龄,66.1[8.5]岁;12931 名[64.1%]男性)和 3265 名 IRIS 参与者(平均[标准差]年龄,62.7[10.6]岁;2151 名[65.9%]男性)。PRoFESS 的中位(IQR)随访时间为 2.4(1.9-3.0)年,IRIS 为 4.7(3.2-5.0)年。在 PRoFESS 中,mRS 为 0 的患者中风复发率为 7.2%,mRS 为 1 或 2 的患者为 8.7%,mRS 为 3 或更高的患者为 10.6%(χ22=27.1;P<0.001);在 IRIS 中,mRS 为 0 的患者中风复发率为 6.4%,mRS 为 1 或 2 的患者为 9.0%,mRS 为 3 或更高的患者为 11.7%(χ22=11.1;P<0.001)。在 PRoFESS 中,mRS 为 0 的患者 MACE 发生率为 10.1%,mRS 为 1 或 2 的患者为 12.2%,mRS 为 3 或更高的患者为 17.2%(χ22=103.4;P<0.001),IRIS 中 mRS 为 0 的患者 MACE 发生率为 10.9%,mRS 为 1 或 2 的患者为 13.3%,mRS 为 3 或更高的患者为 15.3%(χ22=5.8;P=0.06)。与 mRS 为 0 的患者相比,mRS 为 3 或更高的患者在 PRoFESS(风险比[HR],1.63;95%置信区间[CI],1.38-1.92;P<0.001)和 IRIS(HR,1.91;95% CI,1.28-2.86;P=0.002)中发生复发性中风的风险更高。在 PRoFESS(HR,1.90;95% CI,1.66-2.18;P<0.001)和 IRIS(HR,1.45;95% CI,1.03-2.03;P=0.03)中,MACE 的发生风险也更高。
本队列研究发现,中风后残疾程度越高,中风复发和 MACE 的发生率越高。在中风预防试验中纳入更多基线残疾程度较高的患者,可能会提高这些研究的统计效力和普遍性。