Department of Emergency and Critical Care Medicine, Faculty of Medicine, Shimane University, 89-1 Enya-Cho, Izumo, Shimane, 693-8501, Japan.
Laboratories Division, Shimane University Hospital, 89-1 Enya-Cho, Izumo, Shimane, 693-8501, Japan.
BMC Infect Dis. 2024 Jul 29;24(1):744. doi: 10.1186/s12879-024-09660-y.
Clostridioides difficile infection is associated with antibiotic use and manifests as diarrhea; however, emerging cases of fulminant diarrhea caused by binary toxin-producing C. difficile unrelated to prior antibiotic exposure have been reported. Although fulminant colitis caused by C. difficile has been documented, instances of intussusception remain scarce. Here, we present a case of adult intussusception with severe hypokalemia and pneumonia resulting from a community-acquired C. difficile infection in Japan.
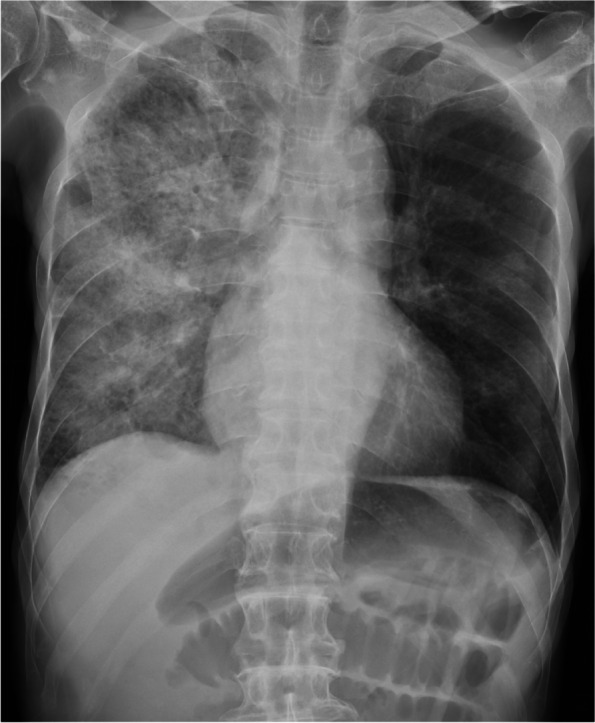
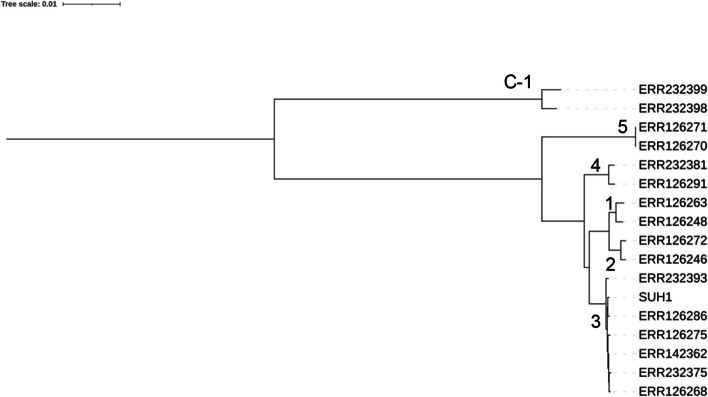
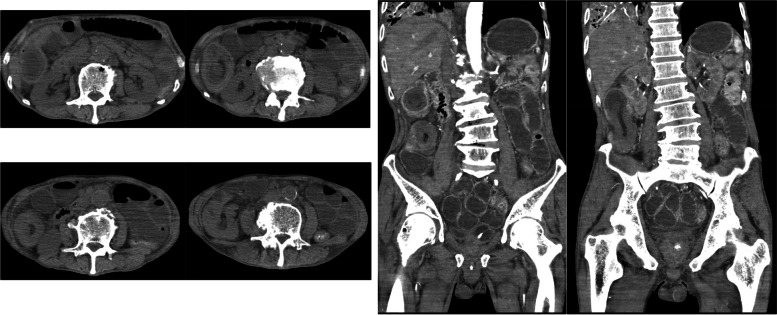
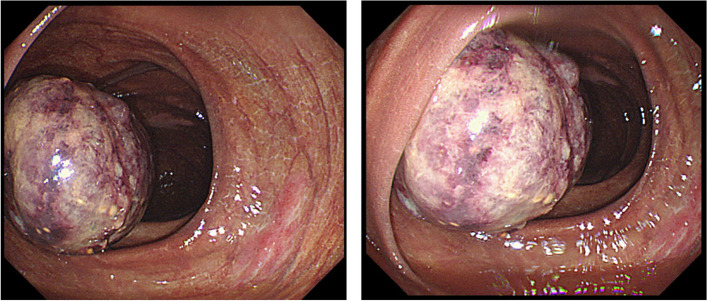
An 82-year-old male presented with dizziness, progressive weakness, and diarrhea. Initial vital signs indicated severe respiratory and circulatory distress, and laboratory findings revealed hypokalemia, pneumonia, and septic shock. Imaging confirmed intussusception of the ascending colon. Although colonoscopy suggested a potential tumor, no malignancy was found. The C. difficile rapid test result was positive, indicating community-acquired C. difficile infection. Treatment with vancomycin was initiated; however, intussusception relapsed. Surgical intervention was successful and led to clinical improvement. The patient's complex pathophysiology involved community-acquired C. difficile-induced severe diarrhea, hypokalemia, hypermetabolic alkalosis, and subsequent intussusception. Although adult intussusception is uncommon, this case was uniquely linked to binary toxin-producing C. difficile. The identified strain, SUH1, belonged to a novel sequence type (ST1105) and clade 3, suggesting a highly virulent clone. Resistome analysis aligned with phenotypic susceptibility to metronidazole and vancomycin, confirming their treatment efficacy.
This case report highlights a binary toxin-producing C. difficile that caused intussusception. The consideration of community-acquired C. difficile in the differential diagnosis of severe enteritis is necessary, even in Japan.
艰难梭菌感染与抗生素使用有关,表现为腹泻;然而,已报道了与先前抗生素暴露无关的产二元毒素艰难梭菌引起的暴发性腹泻的新发病例。虽然有艰难梭菌引起的暴发性结肠炎的记载,但肠套叠的病例仍然很少。在此,我们报告了一例日本社区获得性艰难梭菌感染引起的成人肠套叠,伴有严重低钾血症和肺炎。
一名 82 岁男性因头晕、进行性虚弱和腹泻就诊。初始生命体征表明存在严重的呼吸和循环窘迫,实验室检查结果显示低钾血症、肺炎和感染性休克。影像学检查证实升结肠肠套叠。虽然结肠镜检查提示可能存在肿瘤,但未发现恶性肿瘤。艰难梭菌快速检测结果阳性,提示社区获得性艰难梭菌感染。开始使用万古霉素治疗,但肠套叠复发。手术干预成功,临床状况改善。患者的复杂病理生理学涉及社区获得性艰难梭菌诱导的严重腹泻、低钾血症、高代谢性碱中毒和随后的肠套叠。虽然成人肠套叠并不常见,但本例与产二元毒素的艰难梭菌有关。鉴定的菌株 SUH1 属于新的序列型(ST1105)和 3 型分支,表明是一种高毒力的克隆。耐药组分析与甲硝唑和万古霉素的表型药敏一致,证实了它们的治疗效果。
本病例报告强调了一种产二元毒素的艰难梭菌引起的肠套叠。即使在日本,也需要考虑社区获得性艰难梭菌在严重肠炎的鉴别诊断中的作用。