Adam Hammaad, Bermea Rene S, Yang Ming Ying, Celi Leo Anthony, Ghassemi Marzyeh
Institute for Data Systems and Society, Massachusetts Institute of Technology; Cambridge, Massachusetts 02139, USA.
Division of Pulmonary & Critical Care Medicine, Massachusetts General Hospital; Boston, Massachusetts 02114, USA.
medRxiv. 2024 Jul 16:2024.07.14.24310395. doi: 10.1101/2024.07.14.24310395.
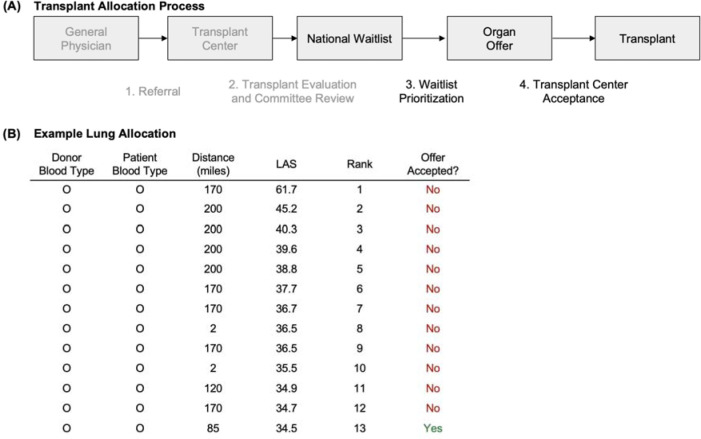
There are known racial disparities in the organ transplant allocation system in the United States. However, prior work has yet to establish if transplant center decisions on offer acceptance-the final step in the allocation process-contribute to these disparities.
To estimate racial differences in the acceptance of organ offers by transplant center physicians on behalf of their patients.
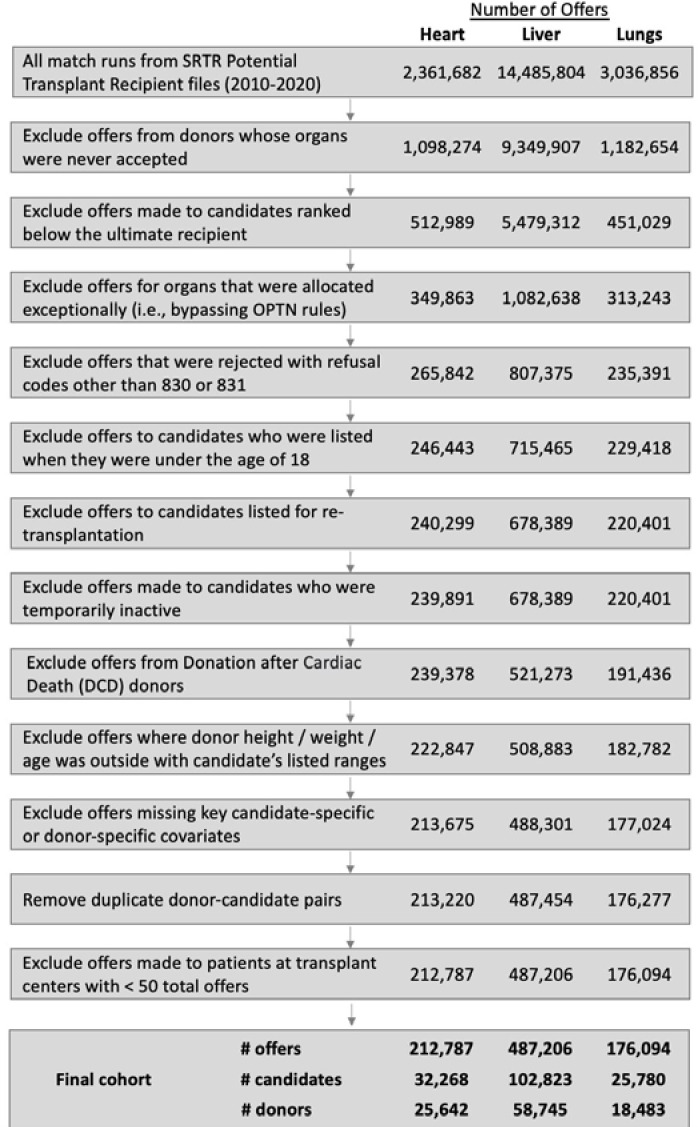
Retrospective cohort analysis using data from the Scientific Registry of Transplant Recipients (SRTR) on patients who received an offer for a heart, liver, or lung transplant between January 1, 2010 and December 31, 2020.
Nationwide, waitlist-based.
32,268 heart transplant candidates, 102,823 liver candidates, and 25,780 lung candidates, all aged 18 or older.
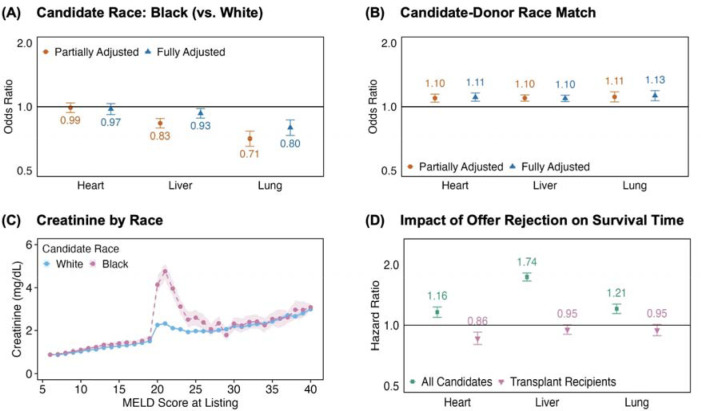
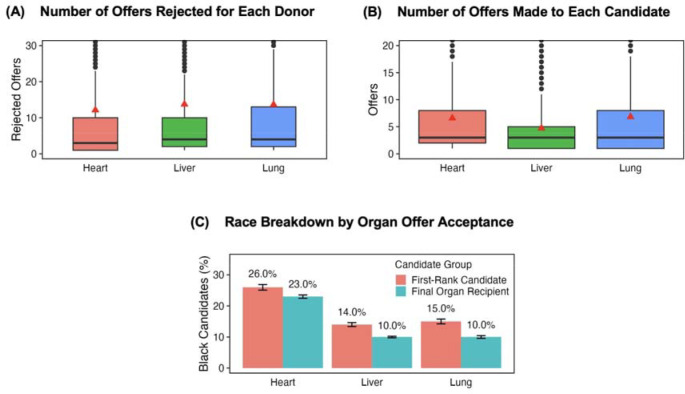
Black race was associated with significantly lower odds of offer acceptance for livers (OR=0.93, CI: 0.88-0.98) and lungs (OR=0.80, CI: 0.73-0.87). Donor-candidate race match was associated with significantly higher odds of offer acceptance for hearts (OR=1.11, CI: 1.06-1.16), livers (OR=1.10, CI: 1.06-1.13), and lungs (OR=1.13, CI: 1.07-1.19). Rejecting an offer was associated with lower survival times for all three organs (heart hazard ratio=1.16, CI: 1.09-1.23; liver HR=1.74, CI: 1.66-1.82; lung HR=1.21, CI: 1.15-1.28).
Our study analyzed the observational SRTR dataset, which has known limitations.
Offer acceptance decisions are associated with inequity in the organ allocation system. Our findings demonstrate the additional barriers that Black patients face in accessing organ transplants and demonstrate the need for standardized practice, continuous distribution policies, and better organ procurement.
在美国的器官移植分配系统中,种族差异是已知的。然而,之前的研究尚未确定移植中心关于接受供体器官的决策(分配过程的最后一步)是否导致了这些差异。
评估移植中心医生代表患者接受器官供体提议方面的种族差异。
采用回顾性队列分析,数据来自移植受者科学注册系统(SRTR),对象为2010年1月1日至2020年12月31日期间收到心脏、肝脏或肺移植提议的患者。
全国范围内,基于等待名单。
32268名心脏移植候选人、102823名肝脏移植候选人以及25780名肺移植候选人,均为18岁及以上。
1)接受提议与两个基于种族的变量之间的关联:候选者种族和供体 - 候选者种族匹配;2)拒绝提议与患者死亡时间之间的关联。
黑人种族与接受肝脏供体提议的几率显著降低相关(OR = 0.93,CI:0.88 - 0.98)以及接受肺供体提议的几率显著降低相关(OR = 0.80,CI:0.73 - 0.87)。供体 - 候选者种族匹配与接受心脏供体提议的几率显著升高相关(OR = 1.11,CI:1.06 - 1.16)、接受肝脏供体提议的几率显著升高相关(OR = 1.10,CI:1.06 - 1.13)以及接受肺供体提议的几率显著升高相关(OR = 1.13,CI:1.07 - 1.19)。拒绝提议与所有三种器官的较低生存时间相关(心脏风险比 = 1.16,CI:1.09 - 1.23;肝脏HR = 1.74,CI:1.66 - 1.82;肺HR = 1.21,CI:1.15 - 1.28)。
我们的研究分析了观察性的SRTR数据集,该数据集存在已知局限性。
接受提议的决策与器官分配系统中的不公平相关。我们的研究结果表明黑人患者在获得器官移植方面面临的额外障碍,并表明需要标准化操作、持续分配政策以及更好的器官获取方式。