Department of Obstetrics and Gynecology, Chang Gung Memorial Hospital at Linkou and Chang Gung University College of Medicine, Taoyuan, Taiwan.
Department of General Surgery, Chang-Gung Memorial Hospital at Linkou, Taoyuan, Taiwan.
Am J Case Rep. 2024 Jul 30;25:e944843. doi: 10.12659/AJCR.944843.
BACKGROUND Endoscopic inguinal hernia repair has become the preferred technique currently. The use of mesh to facilitate a tension-free reinforcement has become the standard of care during endoscopic totally extraperitoneal (TEP), laparoscopic transabdominal pre-peritoneal, and open inguinal hernia repair. Although uncommon, late-developing mesh infections, defined as those occurring in the surgical site months or years after the procedure, can lead to severe complications. To achieve the best possible outcome for the patient, prompt imaging and a multidisciplinary approach to management, including complete surgical removal of the contaminated mesh and proper antibiotic therapy, are crucial. CASE REPORT A 39-year-old woman presented with a 1-month history of intermittent fever, progressive lower abdominal pain and fullness, and purulent discharge from the abdominal wall. Her medical history was significant for an endoscopic right TEP inguinal hernia repair performed 3 years earlier, which involved the use of an anatomic mesh and titanium screws. Physical examination and ultrasound findings revealed a large preperitoneal abscess with cutaneous fistulization, secondary to a deep-seated mesh infection. Pseudomonas aeruginosa was identified as the causative pathogen. She underwent a 2-step surgical procedure, including an initial fistulectomy followed by endoscopic abscess drainage and surgical excision of the infected mesh, combined with antimicrobial therapy, resulting in an excellent clinical response and complete resolution. This strategy also allowed for an effective assessment of the abdominal wall integrity. CONCLUSIONS This case underscores the importance of considering late-developing mesh infections in patients presenting with abdominal symptoms who have previously undergone TEP hernia repair, even years after the initial surgery.
目前,内镜腹股沟疝修补术已成为首选技术。在进行内镜完全腹膜外(TEP)、腹腔镜经腹腹膜前和开放式腹股沟疝修补术时,使用网片来实现无张力加强已经成为护理标准。尽管罕见,但迟发性网片感染(定义为手术后数月或数年后在手术部位发生的感染)可能导致严重并发症。为了使患者获得最佳的治疗效果,及时进行影像学检查并采取多学科管理方法至关重要,包括彻底切除受污染的网片和适当的抗生素治疗。
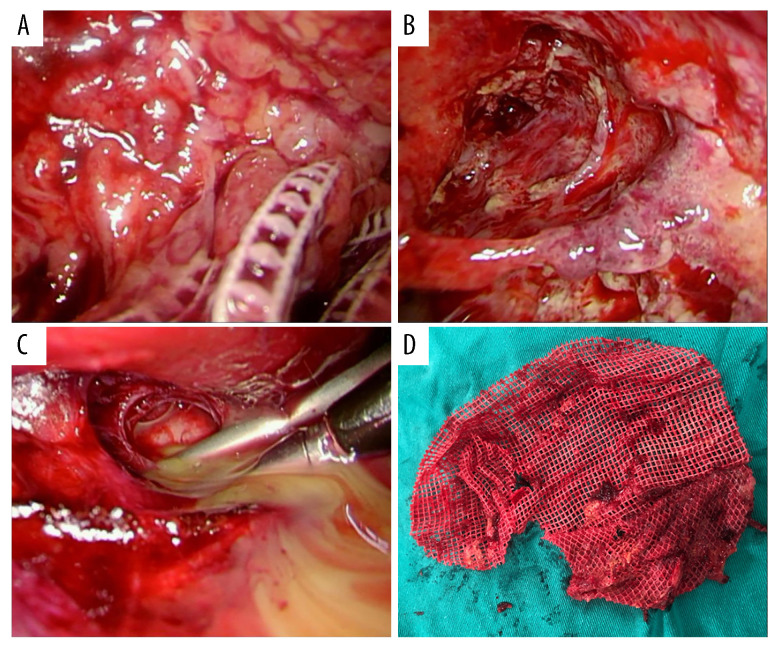
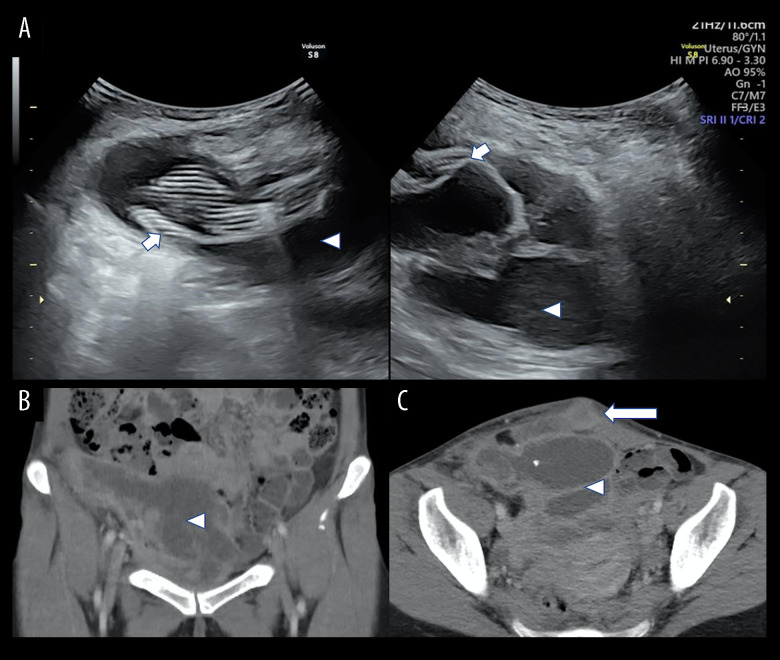
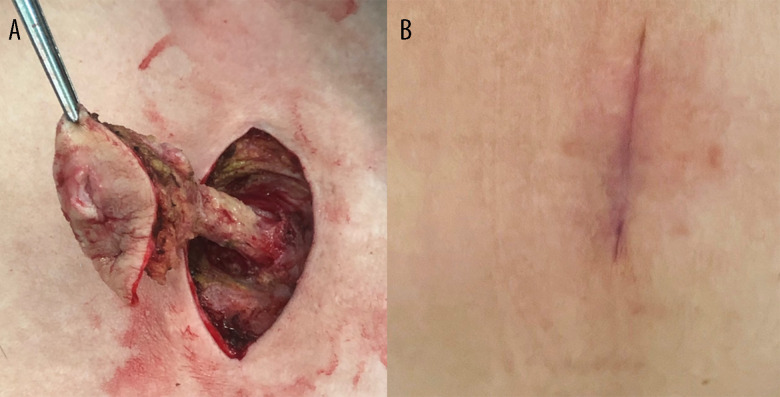
一名 39 岁女性,因间歇性发热、下腹部疼痛和饱胀进行性加重以及腹壁脓性分泌物排出,就诊 1 个月。她的病史包括 3 年前进行的内镜右侧 TEP 腹股沟疝修补术,该手术涉及使用解剖网片和钛钉。体格检查和超声检查结果显示,存在大的腹膜前脓肿,并伴有皮肤瘘管形成,继发于深部网片感染。鉴定出病原体为铜绿假单胞菌。她接受了两步手术治疗,包括初次瘘管切除术,随后进行内镜脓肿引流和感染网片的手术切除,并联合抗菌治疗,取得了极好的临床疗效,完全缓解。这种策略还可以有效地评估腹壁完整性。
本病例强调了对于先前接受过 TEP 疝修补术的患者,即使在初次手术后多年,出现腹部症状时,应考虑迟发性网片感染的重要性。