Ninomiya Kai, Serruys Patrick W, Garg Scot, Hara Hironori, Masuda Shinichiro, Kageyama Shigetaka, Kotoku Nozomi, Sevestre Emelyne, Kumar Abhishek, O'Kane Peter, Zaman Azfar, Farah Bruno, Magro Michael, Oemrawsingh Rohit M, Möllmann Helge, Meneveau Nicolas, Achenbach Stephan, Lemoine Julien, Allali Abdelhakim, Gallagher Sean, Wykrzykowska Joanna, Lesiak Maciej, Silvestri Marc, Wijns William, Sharif Faisal, Onuma Yoshinobu
Department of Cardiology, National University of Ireland, Galway (NUIG), H91 TK33 Galway, Ireland.
Department of Cardiology, Academic Medical Center, University of Amsterdam, 1105 AZ Amsterdam, The Netherlands.
Rev Cardiovasc Med. 2022 Apr 8;23(4):133. doi: 10.31083/j.rcm2304133. eCollection 2022 Apr.
Personalized prognosis plays a vital role in deciding between percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG) in patients with three-vessel disease (3VD). The aim of this study is to compare the modality of revascularization chosen by the local heart team to that recommended by using individualized predictions of medium, and long-term all-cause mortality amongst patients with 3VD screened in the Multivessel TALENT trial.
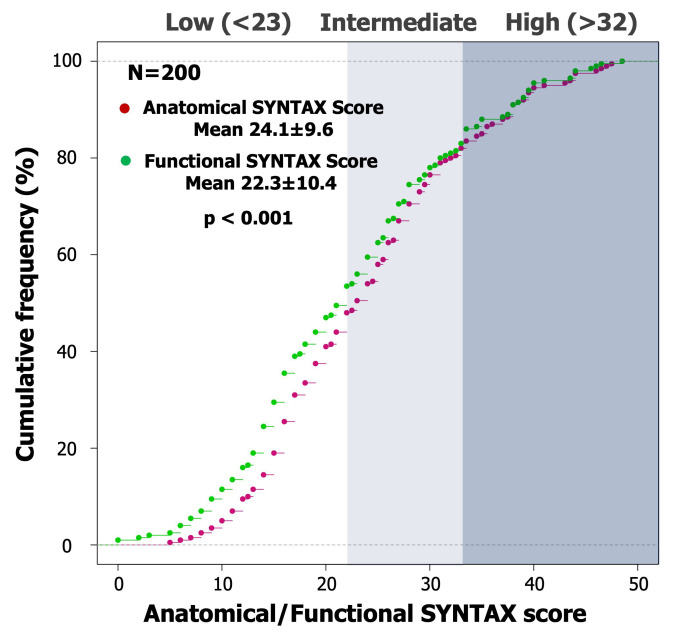
The SYNTAX score II (SS-II) and SS-2020 were evaluated in 200 consecutive patients by a core laboratory and compared to the decision of the "on site" heart team.
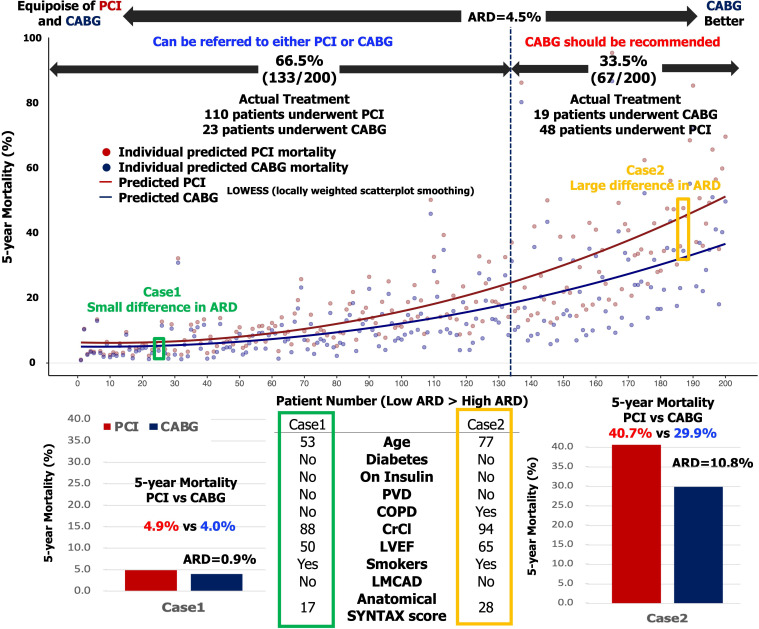
According to the SS-II, CABG was the recommended treatment in 51 patients (25.5%) however 34 (66.6%) of them received PCI. According to SS-2020 the predicted absolute risk differences (ARD) between PCI and CABG were significantly higher in patients receiving CABG compared to those treated by PCI for major adverse cardiovascular and cerebrovascular events, a composite of all-cause mortality, stroke or myocardial infarction at 5-years (8.8 4.6% vs 6.0 4.0%, 0.001) and all-cause mortality at 5- (5.2 3.5% vs 3.7 3.0%, = 0.008) and 10-years (9.3 4.8% vs 6.2 4.2%, 0.001). Based on the novel threshold of equipoise (individual absolute risk differences [ARD] 4.5%), 133 patients were eligible for PCI however 23 of them underwent CABG; conversely, amongst the 67 patients where CABG was recommendation (individual ARD 4.5%), only 19 received it.
Despite the robustness of the risk models proposed for screening, several deviations from the recommended mode of revascularization were observed by the core laboratory among the first 200 patients with 3VD screened in the Multivessel TALENT trial.
ClinicalTrials.gov reference: NCT04390672.
在三支血管病变(3VD)患者中,个性化预后对于决定采用经皮冠状动脉介入治疗(PCI)还是冠状动脉旁路移植术(CABG)起着至关重要的作用。本研究的目的是比较在多支血管病变TALENT试验中筛选出的3VD患者中,当地心脏团队选择的血运重建方式与使用中期和长期全因死亡率的个体化预测所推荐的方式。
由一个核心实验室对连续200例患者进行SYNTAX评分II(SS-II)和SS-2020评估,并与“现场”心脏团队的决策进行比较。
根据SS-II,51例患者(25.5%)推荐行CABG,但其中34例(66.6%)接受了PCI。根据SS-2020,在接受CABG的患者中,与接受PCI的患者相比,PCI和CABG之间预测的主要不良心血管和脑血管事件的绝对风险差异(ARD)显著更高,主要不良心血管和脑血管事件是5年时全因死亡率、中风或心肌梗死的综合指标(8.8±4.6%对6.0±4.0%,P=0.001)以及5年(5.2±3.5%对3.7±3.0%,P=0.008)和10年(9.3±4.8%对6.2±4.2%,P=0.001)时的全因死亡率。基于新的平衡阈值(个体绝对风险差异[ARD]≥4.5%),133例患者适合行PCI,但其中23例接受了CABG;相反,在推荐行CABG的67例患者(个体ARD≥4.5%)中,只有19例接受了CABG。
尽管所提出的用于筛选的风险模型具有稳健性,但在多支血管病变TALENT试验中筛选出的首批200例3VD患者中,核心实验室观察到与推荐的血运重建方式存在一些偏差。
ClinicalTrials.gov标识符:NCT04390672。