Department of Cardiology, John Radcliffe Hospital, Oxford University Hospitals, Headley Way, Oxford OX3 9DU, UK.
Department of Cardiology, National University of Ireland, Galway, Ireland.
Eur Heart J. 2022 Mar 31;43(13):1307-1316. doi: 10.1093/eurheartj/ehab703.
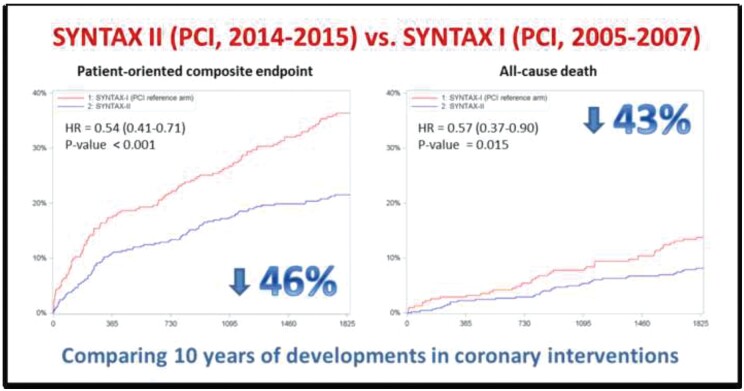
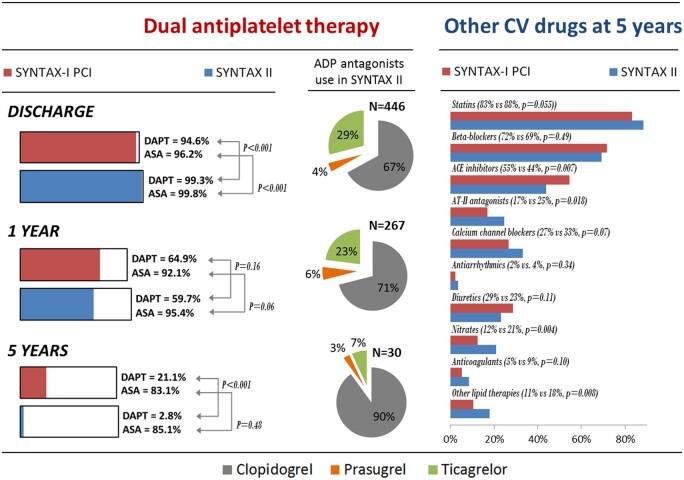
The SYNTAX II study evaluated the impact of advances in percutaneous coronary intervention (PCI), integrated into a single revascularization strategy, on outcomes of patients with de novo three-vessel disease. The study employed decision-making utilizing the SYNTAX score II, use of coronary physiology, thin-strut biodegradable polymer drug-eluting stents, intravascular ultrasound, enhanced treatments of chronic total occlusions, and optimized medical therapy. Patients treated with this approach were compared with predefined patients from the SYNTAX I trial.
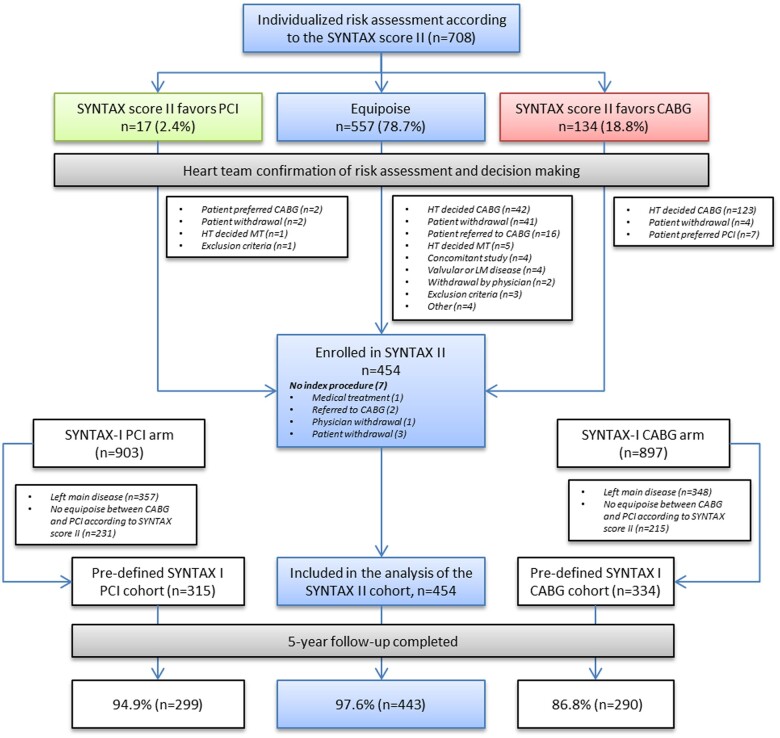
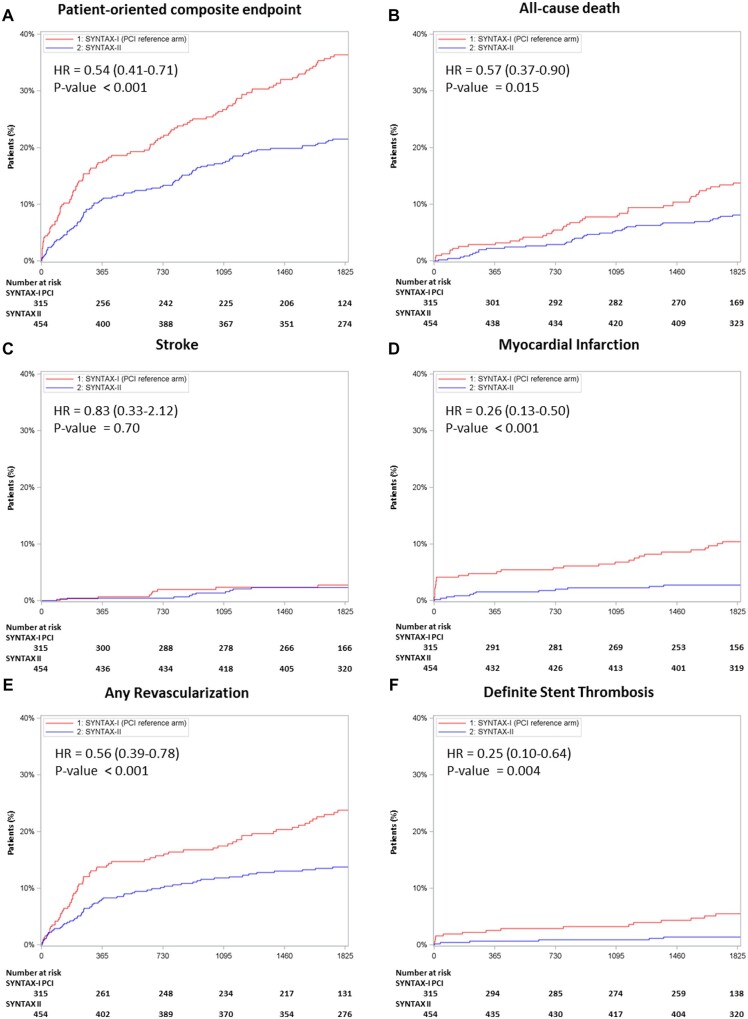
SYNTAX II was a multicentre, single-arm, open-label study of patients requiring revascularization who demonstrated clinical equipoise for treatment with either coronary artery bypass grafting (CABG) or PCI, predicted by the SYNTAX score II. The primary endpoint was major adverse cardiac and cerebrovascular events (MACCE), which included any revascularization. The comparators were a matched PCI cohort trial and a matched CABG cohort, both from the SYNTAX I trial. At 5 years, MACCE rate in SYNTAX II was significantly lower than in the SYNTAX I PCI cohort (21.5% vs. 36.4%, P < 0.001). This reflected lower rates of revascularization (13.8% vs. 23.8%, P < 0.001), and myocardial infarction (MI) (2.7% vs. 10.4%, P < 0.001), consisting of both procedural MI (0.2% vs. 3.8%, P < 0.001) and spontaneous MI (2.3% vs. 6.9%, P = 0.004). All-cause mortality was lower in SYNTAX II (8.1% vs. 13.8%, P = 0.013) reflecting a lower rate of cardiac death (2.8% vs. 8.4%, P < 0.001). Major adverse cardiac and cerebrovascular events' outcomes at 5 years among patients in SYNTAX II and predefined patients in the SYNTAX I CABG cohort were similar (21.5% vs. 24.6%, P = 0.35).
Use of the SYNTAX II PCI strategy in patients with de novo three-vessel disease led to improved and durable clinical results when compared to predefined patients treated with PCI in the original SYNTAX I trial. A predefined exploratory analysis found no significant difference in MACCE between SYNTAX II PCI and matched SYNTAX I CABG patients at 5-year follow-up.
SYNTAX II 研究评估了经皮冠状动脉介入治疗(PCI)的进展,将其整合到单一血运重建策略中,对新发三血管疾病患者的结局的影响。该研究采用 SYNTAX II 评分进行决策,利用冠状动脉生理学、薄支架生物可降解聚合物药物洗脱支架、血管内超声、慢性完全闭塞的强化治疗以及优化的药物治疗。接受这种方法治疗的患者与来自 SYNTAX I 试验的预定患者进行了比较。
SYNTAX II 是一项多中心、单臂、开放标签的研究,纳入了需要血运重建的患者,这些患者在 SYNTAX II 评分预测下,对冠状动脉旁路移植术(CABG)或 PCI 治疗具有临床均势。主要终点是主要不良心脏和脑血管事件(MACCE),包括任何血运重建。对照组是来自 SYNTAX I 试验的匹配 PCI 队列试验和匹配 CABG 队列。在 5 年时,SYNTAX II 中的 MACCE 发生率明显低于 SYNTAX I PCI 队列(21.5% vs. 36.4%,P < 0.001)。这反映了较低的血运重建率(13.8% vs. 23.8%,P < 0.001)和心肌梗死(MI)率(2.7% vs. 10.4%,P < 0.001),包括操作相关 MI(0.2% vs. 3.8%,P < 0.001)和自发性 MI(2.3% vs. 6.9%,P = 0.004)。SYNTAX II 的全因死亡率较低(8.1% vs. 13.8%,P = 0.013),反映了较低的心脏死亡率(2.8% vs. 8.4%,P < 0.001)。SYNTAX II 中 5 年的主要不良心脏和脑血管事件结局与 SYNTAX I CABG 队列中预定患者的结局相似(21.5% vs. 24.6%,P = 0.35)。
在新发三血管疾病患者中使用 SYNTAX II PCI 策略与原始 SYNTAX I 试验中接受 PCI 治疗的预定患者相比,可改善并维持临床结果。一项预设的探索性分析发现,5 年随访时,SYNTAX II PCI 与匹配的 SYNTAX I CABG 患者的 MACCE 无显著差异。