Matta Anthony, Campelo-Parada Francisco, Nader Vanessa, Lhermusier Thibault, Bouisset Frédéric, Blanco Stéphanie, Elbaz Meyer, Roncalli Jerome, Carrié Didier
Department of Cardiology, Toulouse University Hospital (Hopital Rangeuil), 31400 Toulouse, France.
Department of Cardiology, Centre Hospitalier Intercommunal Castres-Mazamet, 81108 Castres, France.
Rev Cardiovasc Med. 2022 Aug 10;23(8):281. doi: 10.31083/j.rcm2308281. eCollection 2022 Aug.
Up to date, the management of coronary artery aneurysm (CAA) is not well defined and depends on local heart team decision. Data reported in literature are scarce and controversial. We aim to compare the long-term outcomes of different therapeutic strategies of CAA (medical vs percutaneous coronary intervention (PCI) vs coronary artery bypass graft(CABG)).
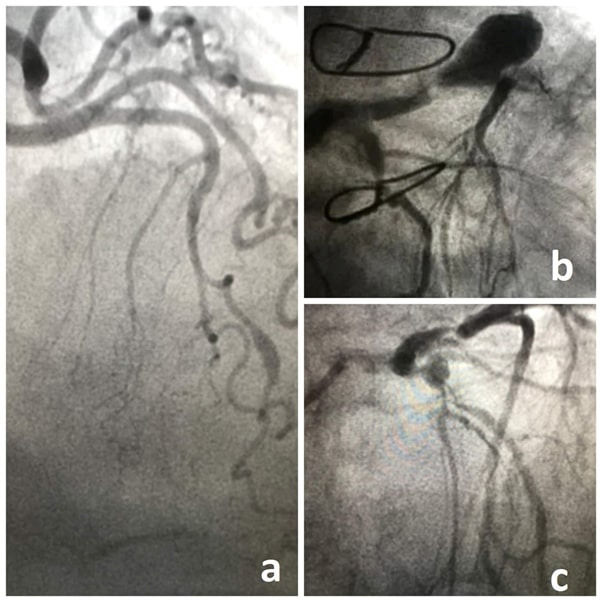
A retrospective cohort study was conducted on 100 consecutive patients who underwent coronary angiography at Toulouse University Hospital, Toulouse France and fulfilled the diagnostic criteria of CAA. Coronary angiograms were reviewed, and all necessary data were collected. CAA was defined by a coronary dilation exceedingly at least 50% of reference coronary diameter.
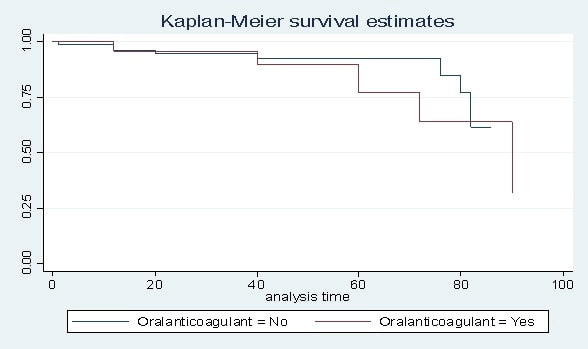
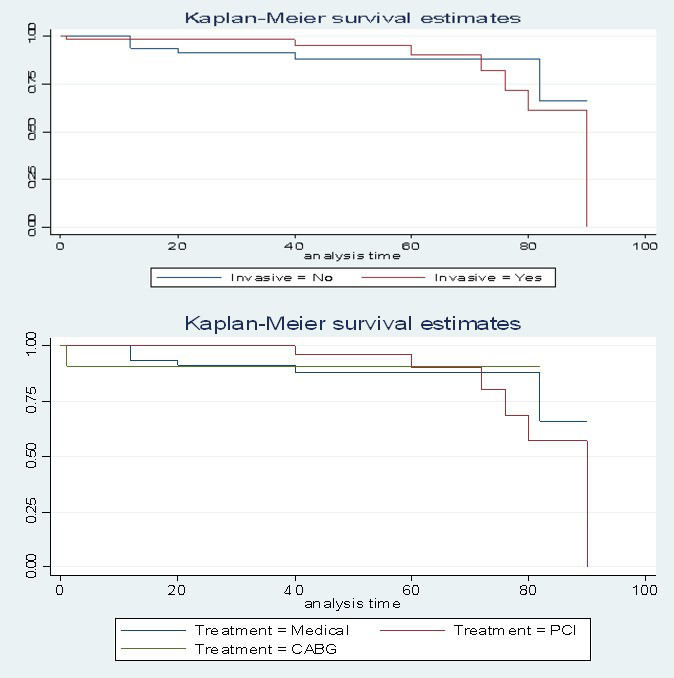
We identified 100 patients with CAA with a mean age of 67.9 12 years. The left anterior descending coronary artery was most affected (36%). CAA is associated with significant coronary artery disease in 78% of cases. The incidence of major adverse cardiovascular and cerebrovascular events (MACCE) was 13% during a median follow-up period of 46.2 24 months. A 53% of patients underwent PCI or CABG. The rate of MACCE was lower in CABG group (9.1%) compared to PCI (14.3%) and medical (12.8%) groups, but without reaching statistically significant level. Longitudinal aneurysm diameter was positively linked to MACCE [OR = 1.109, 95% CI (1.014-1.214), = 0.024]. No benefits have been attributed to anticoagulant regimen over antiplatelet therapy.
In our retrospective observational study, there seems to be no significant differences in MACCE-free survival between all groups (Medical vs PCI vs CABG). Larger longitudinal aneurysm diameter was identified as a predictor of poor prognosis during follow-up.
到目前为止,冠状动脉瘤(CAA)的管理尚未明确界定,取决于当地心脏团队的决策。文献报道的数据稀少且存在争议。我们旨在比较CAA不同治疗策略(药物治疗与经皮冠状动脉介入治疗(PCI)与冠状动脉旁路移植术(CABG))的长期疗效。
对在法国图卢兹大学医院接受冠状动脉造影且符合CAA诊断标准的100例连续患者进行了一项回顾性队列研究。回顾冠状动脉造影,并收集所有必要数据。CAA定义为冠状动脉扩张超过参考冠状动脉直径的至少50%。
我们确定了100例CAA患者,平均年龄为67.9±12岁。左前降支冠状动脉受累最严重(36%)。78%的病例中CAA与严重冠状动脉疾病相关。在中位随访期46.2±24个月期间,主要不良心血管和脑血管事件(MACCE)的发生率为13%。53%的患者接受了PCI或CABG。与PCI组(14.3%)和药物治疗组(12.8%)相比,CABG组的MACCE发生率较低(9.1%),但未达到统计学显著水平。纵向动脉瘤直径与MACCE呈正相关[比值比=1.109,95%置信区间(1.014 - 1.214),P = = 0.024]。与抗血小板治疗相比,抗凝方案未显示出益处。
在我们的回顾性观察研究中,所有组(药物治疗组与PCI组与CABG组)之间无MACCE生存情况似乎没有显著差异。较大的纵向动脉瘤直径被确定为随访期间预后不良的预测因素。