So Sarah, Lei Li Kelly Chen
Department of Renal Medicine, Nepean Kidney Research Center, Nepean Hospital, Kingswood, Sydney, New South Wales, Australia.
The University of Sydney, Sydney, New South Wales, Australia.
Kidney Int Rep. 2024 Apr 24;9(7):2117-2124. doi: 10.1016/j.ekir.2024.04.045. eCollection 2024 Jul.
Dialysis withdrawal represents an increasingly common cause of death in patients receiving kidney replacement therapy internationally. Prognostic information about stopping dialysis guides clinicians counseling patients and families regarding end-of-life care. However, few studies examine prognostication after withdrawal. We aimed to determine median survival time after withdrawal of dialysis, and to determine which patient and dialysis-related factors are significantly associated with prognosis.
This retrospective cohort study used registry data. We included all adult patients from the Western Renal Services who were receiving peritoneal dialysis (PD) or hemodialysis prior to death, whose cause of death was documented as "withdrawal from dialysis" and whose date of death was between January 1, 2016 and June 30, 2022. Demographic, clinical, and biochemical data was extracted. The primary outcome was time-to-death, defined as days from last dialysis session to date of death.
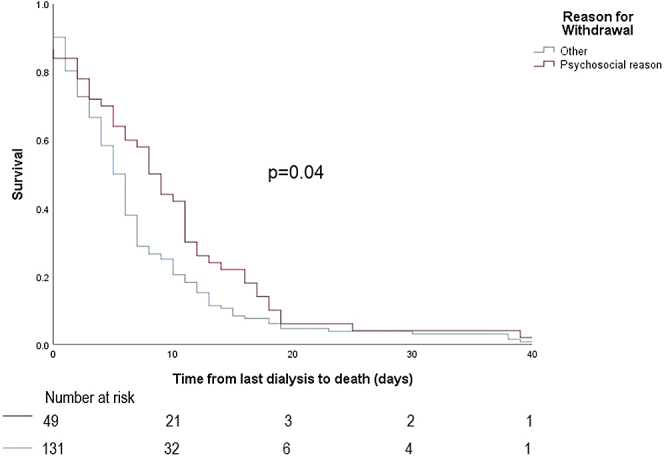
Median survival time from last dialysis to death for the PD group ( = 53) was 4 days (interquartile range [IQR]: 3-10 days), not significantly different from the hemodialysis group which was 6 days (IQR: 2-11 days, = 0.72). For PD, the only variable significantly associated with survival time was reason for withdrawing ( = 0.01). Median survival time was significantly longer for patients withdrawing for psychosocial reasons compared to those withdrawing for other reasons ( = 0.002). For hemodialysis ( = 186), variables significantly associated with survival time from last dialysis to death was reason for withdrawing ( = 0.001), urine production at the time of withdrawal ( = 0.005), serum sodium ( = 0.02) and smoking status ( = 0.009).
Median survival time was longer for withdrawals for psychosocial reasons compared to medical reasons. The data presented could inform withdrawal discussions regarding prognostication and end-of-life planning with patients and family.
在国际上接受肾脏替代治疗的患者中,停止透析是一种越来越常见的死亡原因。关于停止透析的预后信息可为临床医生就临终关怀向患者及其家属提供咨询提供指导。然而,很少有研究探讨停止透析后的预后情况。我们旨在确定停止透析后的中位生存时间,并确定哪些患者及与透析相关的因素与预后显著相关。
这项回顾性队列研究使用了登记数据。我们纳入了西部肾脏服务中心所有在死亡前接受腹膜透析(PD)或血液透析的成年患者,其死亡原因记录为“停止透析”,且死亡日期在2016年1月1日至2022年6月30日之间。提取了人口统计学、临床和生化数据。主要结局是死亡时间,定义为从最后一次透析 session 到死亡日期的天数。
PD组(n = 53)从最后一次透析到死亡的中位生存时间为4天(四分位间距[IQR]:3 - 10天),与血液透析组的6天(IQR:2 - 11天,n = 0.72)无显著差异与之相比,对于PD,唯一与生存时间显著相关的变量是停止透析的原因(P = 0.01)。因社会心理原因停止透析的患者中位生存时间明显长于因其他原因停止透析的患者(P = 0.002)。对于血液透析(n = 186),与从最后一次透析到死亡的生存时间显著相关的变量是停止透析的原因(P = 0.001)、停止透析时的尿量(P = 0.005)、血清钠(P = 0.02)和吸烟状况(P = 0.009)。
因社会心理原因停止透析的患者中位生存时间比因医疗原因停止透析的患者长。所呈现的数据可为与患者及其家属就预后和临终规划进行停止透析的讨论提供参考。