Walsh Jessica A, Lin Iris, Zhao Ruizhi, Shiff Natalie J, Morrison Laura, Emond Bruno, Yu Louise H, Schwartzbein Samuel, Lefebvre Patrick, Pilon Dominic, Chakravarty Soumya D, Mease Philip
University of Utah School of Medicine, 50 North Medical Drive, Salt Lake City, UT, 84132, US.
Salt Lake City Veterans Affairs Health, Salt Lake City, Utah, US.
Drugs Real World Outcomes. 2024 Sep;11(3):487-499. doi: 10.1007/s40801-024-00428-z. Epub 2024 Jul 31.
Treatment persistence among patients with psoriatic arthritis (PsA) is essential for achieving optimal treatment outcomes. Guselkumab, a fully human interleukin-23p19-subunit inhibitor, was approved by the United States (US) Food and Drug Administration for the treatment of active PsA in July 2020, with a dosing regimen of 100 mg at week 0, week 4, then every 8 weeks. In the Phase 3 DISCOVER-1 and DISCOVER-2 studies of patients with active PsA, 94% of guselkumab-randomized patients completed treatment through 1 year and 90% did so through 2 years (DISCOVER-2). Real-world evidence is needed to compare treatment persistence while following US prescribing guidelines (i.e., on-label persistence) for guselkumab versus subcutaneous (SC) tumor necrosis factor inhibitors (TNFis).
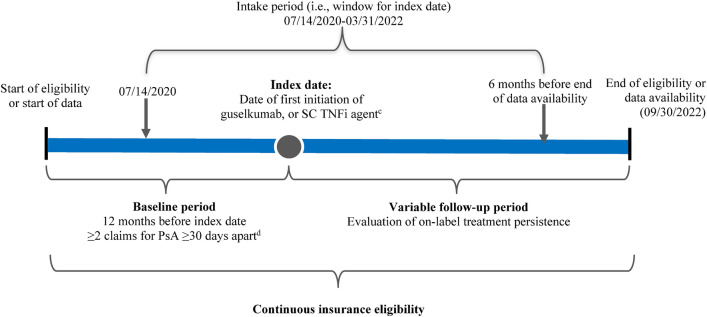
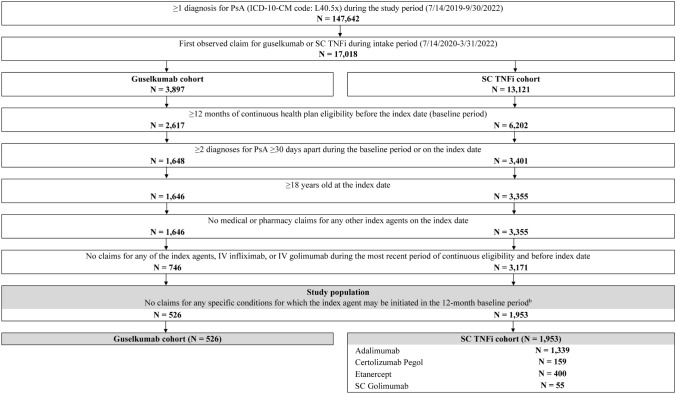
Adults with PsA receiving guselkumab or their first SC TNFi (i.e., adalimumab, certolizumab pegol, etanercept, or golimumab) between 14 July 2020 and 31 March 2022 were identified in the IQVIA PharMetrics Plus database (first claim defined the treatment start date [index date]). Baseline characteristics and biologic use (biologic-naïve/biologic-experienced) were assessed during the 12-month period preceding the index date. Baseline characteristics were balanced between cohorts using propensity-score weighting based on the standardized mortality ratio approach. The follow-up period spanned from the index date until the earlier of the end of continuous insurance eligibility or end of data availability. On-label persistence, defined as the absence of treatment discontinuation (based on a gap of 112 days for guselkumab or 56 days for SC TNFi) or any dose escalation/reduction during follow-up, was assessed in the weighted treatment cohorts using Kaplan-Meier (KM) curves. A Cox proportional hazards model, further adjusted for baseline biologic use, was used to compare on-label persistence between the weighted cohorts.
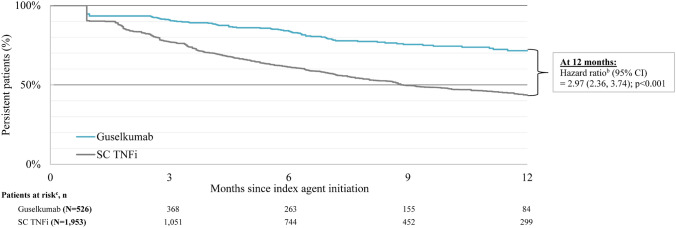
The guselkumab cohort included 526 patients (mean age 49.8 years; 61.2% female) and the SC TNFi cohort included 1953 patients (mean age: 48.5 years; 60.2% female). After weighting, baseline characteristics were well balanced with a mean follow-up of 12.3-12.4 months across cohorts; 51.5% of patients in the guselkumab cohort and 16.7% in the SC TNFi cohort received biologics in the 12-month baseline period. Respective rates of treatment persistence at 3, 6, 9, and 12 months were 91.2%, 84.1%, 75.9%, and 71.5% for the guselkumab cohort versus 77.3%, 61.6%, 50.0%, and 43.7% for the SC TNFi cohort (all log-rank p < 0.001). At 12 months, patients in the guselkumab cohort were 3.0 times more likely than patients in the SC TNFi cohort to remain persistent on treatment (p < 0.001). Median time to discontinuation was not reached for the guselkumab cohort and was 8.9 months for the SC TNFi cohort.
This real-world study employing US commercial health-plan claims data to assess on-label treatment persistence in PsA demonstrated that, at 12 months, guselkumab was associated with a 3 times greater likelihood of persistence compared with SC TNFi.
银屑病关节炎(PsA)患者的治疗持续性对于实现最佳治疗效果至关重要。古塞库单抗是一种全人源白细胞介素-23p19亚基抑制剂,于2020年7月获得美国食品药品监督管理局批准用于治疗活动性PsA,给药方案为第0周、第4周各注射100mg,之后每8周注射一次。在活动性PsA患者的3期DISCOVER-1和DISCOVER-2研究中,94%接受古塞库单抗随机分组的患者完成了1年的治疗,90%的患者完成了2年的治疗(DISCOVER-2)。需要真实世界证据来比较遵循美国处方指南(即标签内持续性)使用古塞库单抗与皮下注射(SC)肿瘤坏死因子抑制剂(TNFis)时的治疗持续性。
在IQVIA PharMetrics Plus数据库中识别出2020年7月14日至2022年3月31日期间接受古塞库单抗或其首个SC TNFis(即阿达木单抗、赛妥珠单抗、依那西普或戈利木单抗)治疗的PsA成年患者(首次索赔确定治疗开始日期[索引日期])。在索引日期前的12个月期间评估基线特征和生物制剂使用情况(初治/曾使用生物制剂)。基于标准化死亡率方法,采用倾向评分加权使各队列间的基线特征达到平衡。随访期从索引日期开始,直至连续保险资格结束或数据可用结束两者中较早的时间点。在加权治疗队列中,使用Kaplan-Meier(KM)曲线评估标签内持续性,定义为随访期间无治疗中断(基于古塞库单抗112天的间隔或SC TNFis 56天的间隔)或任何剂量增加/减少。使用进一步根据基线生物制剂使用情况进行调整的Cox比例风险模型比较加权队列间的标签内持续性。
古塞库单抗队列包括526例患者(平均年龄49.8岁;61.2%为女性),SC TNFis队列包括1953例患者(平均年龄:48.5岁;60.2%为女性)。加权后,各队列间基线特征达到良好平衡,平均随访时间为12.3 - 12.4个月;古塞库单抗队列中51.5%的患者和SC TNFis队列中16.7%的患者在12个月的基线期接受了生物制剂治疗。古塞库单抗队列在3、6、9和12个月时的治疗持续性分别为91.2%、84.1%、75.9%和71.5%,而SC TNFis队列分别为77.3%、61.6%、50.0%和43.7%(所有对数秩检验p < 0.001)。在12个月时,古塞库单抗队列中的患者持续治疗的可能性是SC TNFis队列中患者的3.0倍(p < 0.001)。古塞库单抗队列未达到停药的中位时间,SC TNFis队列的中位停药时间为8.9个月。
这项利用美国商业健康保险理赔数据评估PsA标签内治疗持续性的真实世界研究表明,在12个月时,与SC TNFis相比,古塞库单抗的持续性可能性高3倍。