Song Yan, Betts Keith A, Lu Yichen, Singh Rakesh, Clewell Jerry, Griffith Jenny
Analysis Group, Boston, MA, USA.
AbbVie Inc., North Chicago, IL, USA.
Rheumatol Ther. 2019 Jun;6(2):285-297. doi: 10.1007/s40744-019-0158-2. Epub 2019 May 4.
Patients with psoriatic arthritis (PsA) who receive an initial tumor necrosis factor inhibitor (TNFi) may switch to another TNFi or a non-TNFi biologic therapy. This study compared the healthcare resource use (HRU), expenditures, and time to discontinuation among TNFi-experienced patients with PsA who switched to different biologic therapies in the United States (US).
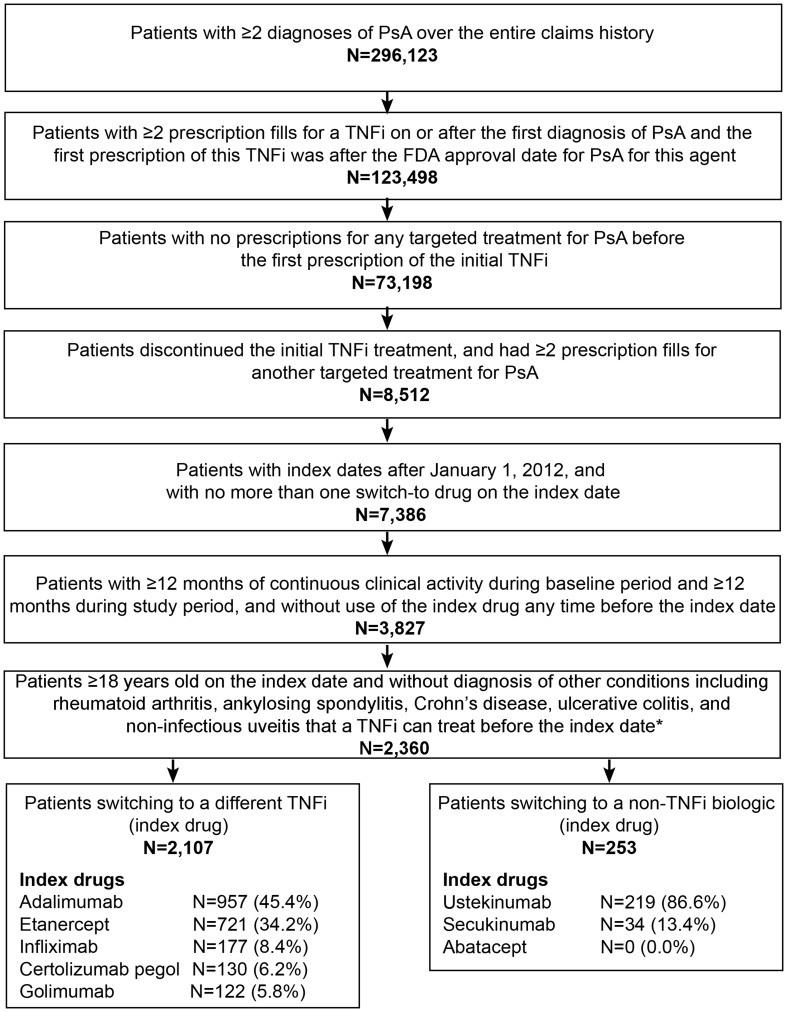
Adults with PsA who discontinued an initial TNFi (adalimumab, etanercept, infliximab, golimumab, or certolizumab pegol) and switched to another TNFi or a non-TNFi (ustekinumab or secukinumab) were identified in the Symphony Health Solutions database [Quarter (Q)1 2010-Q2 2017]. Eligible patients had claims data activity for ≥ 12 months before (baseline) and after (study period) the switching date. All-cause HRU, costs (2017 US dollars), and time to discontinuation during the study period were compared between patients switching to another TNFi vs. a non-TNFi (index drug). Multivariable regression models adjusted for baseline covariates (index year, age, sex, initial TNFi, comorbidities, baseline HRU, and PsA-related treatment history).
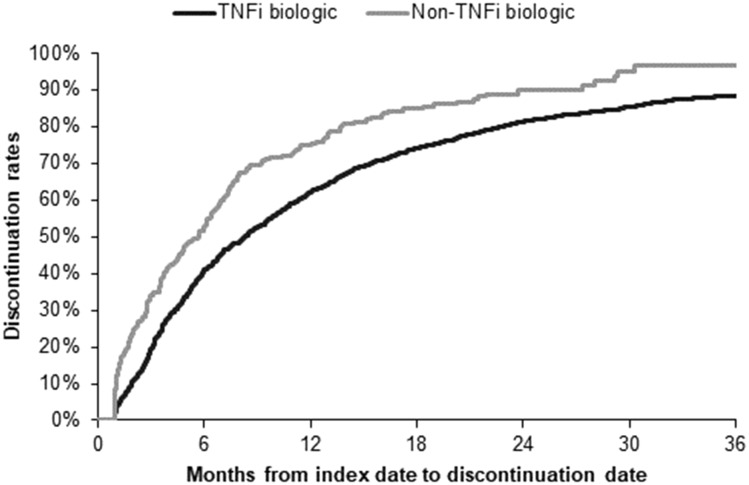
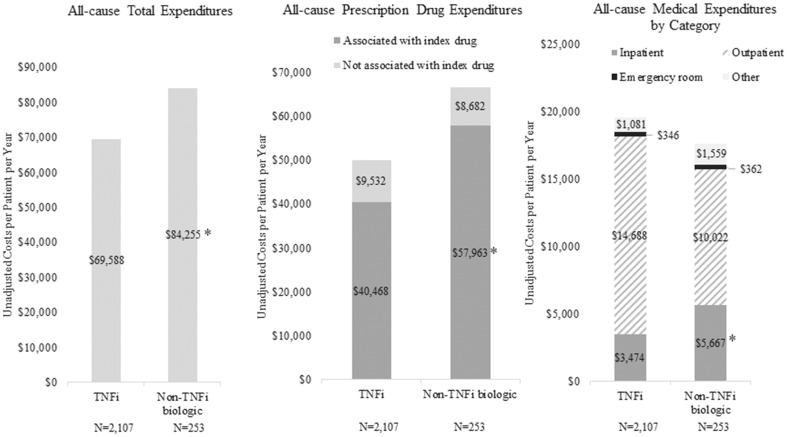
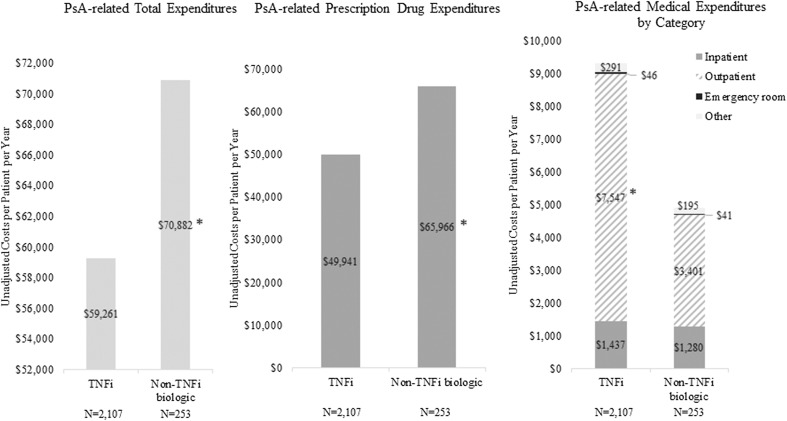
Of 2107 patients switching to another TNFi and 253 switching to a non-TNFi, adalimumab and etanercept were the most common initial TNFi in both cohorts. During the study period, patients switching to another TNFi had significantly fewer dermatologists visits (0.43; p < 0.01) but more rheumatologist visits (1.56, p < 0.01) than patients switching to a non-TNFi. Patients switching to another TNFi vs. a non-TNFi incurred significantly lower total average healthcare expenditures (adjusted difference: $17,625; p < 0.01), driven by lower prescription drug (adjusted difference: $17,172; p < 0.01) and hospitalization expenditures (adjusted difference: $5772; p = 0.04). Patients who switched to another TNFi vs. a non-TNFi continued on their index therapy significantly longer (median time to discontinuation: 8.31 vs. 5.68 months; log-rank p < 0.01).
Patients with PsA who switched to another TNFi had lower total healthcare expenditures and longer persistence compared with patients who switched to a non-TNFi biologic.
AbbVie.
接受初始肿瘤坏死因子抑制剂(TNFi)治疗的银屑病关节炎(PsA)患者可能会换用另一种TNFi或非TNFi生物疗法。本研究比较了美国PsA患者中,换用不同生物疗法的TNFi经验丰富患者的医疗资源使用(HRU)、支出以及停药时间。
在Symphony Health Solutions数据库(2010年第1季度 - 2017年第2季度)中识别出停用初始TNFi(阿达木单抗、依那西普、英夫利昔单抗、戈利木单抗或赛妥珠单抗)并换用另一种TNFi或非TNFi(乌司奴单抗或司库奇尤单抗)的成年PsA患者。符合条件的患者在换药日期之前(基线)和之后(研究期)有≥12个月的索赔数据活动。比较换用另一种TNFi与换用非TNFi(索引药物)的患者在研究期内的全因HRU、成本(2017美元)和停药时间。多变量回归模型针对基线协变量(索引年份、年龄、性别、初始TNFi、合并症、基线HRU和PsA相关治疗史)进行了调整。
在2107例换用另一种TNFi的患者和253例换用非TNFi的患者中,阿达木单抗和依那西普是两个队列中最常见的初始TNFi。在研究期内,换用另一种TNFi的患者皮肤科就诊次数显著较少(0.43;p < 0.01),但风湿病科就诊次数多于换用非TNFi的患者(1.56,p < 0.01)。与换用非TNFi的患者相比,换用另一种TNFi的患者总平均医疗支出显著更低(调整差异:17,625美元;p < 0.01),这是由较低的处方药支出(调整差异:17,172美元;p < 0.01)和住院支出(调整差异:5772美元;p = 0.04)驱动的。换用另一种TNFi与换用非TNFi的患者继续接受索引治疗的时间显著更长(中位停药时间:8.31个月对5.68个月;对数秩检验p < 0.01)。
与换用非TNFi生物疗法的患者相比,换用另一种TNFi的PsA患者总医疗支出更低且持续用药时间更长。
艾伯维公司。