Réanimation Polyvalente, Centre Hospitalier Universitaire Felix Guyon La Réunion, Saint Denis, France.
Soins intensifs néphrologiques et rein aigu, Hôpital Tenon, Paris, France.
Medicine (Baltimore). 2024 Aug 2;103(31):e38986. doi: 10.1097/MD.0000000000038986.
Pink urine syndrome is a rare, poorly understood condition, often prompted by obesity, insulin resistance, and the drug propofol. It is characterized by pink urine or urine sediment and occurs in the absence of a heme or food-based pigment. The pathophysiology of this syndrome is not yet fully understood but is linked to a uric acid metabolism disorder. Pink urine syndrome is less familiar to anesthesiologists than other propofol infusion complications. Our case report aims to highlight this rarely encountered syndrome, whose both diagnosis and therapeutic may be challenging. We have reported the first case of this syndrome evidenced by the change in color of the effluent bag during continuous veno-venous hemofiltration (CVVHF).
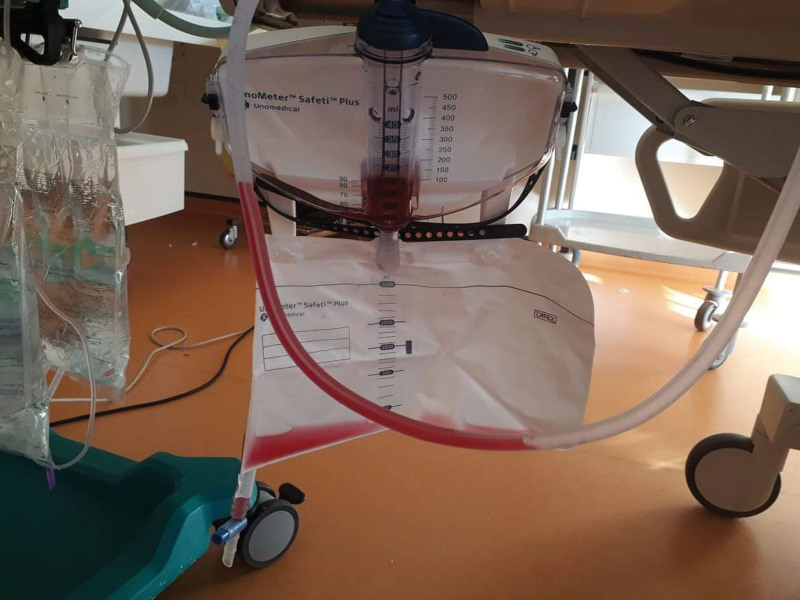
A 61-year-old woman was admitted to the intensive care unit following a recovered cardiorespiratory arrest due to ventricular arrhythmia. She was placed in hypothermia, sedated with propofol (300 mg/h), and started on CVVHF for oligo-anuric acute kidney injury associated with severe metabolic acidosis. A few hours after initiation of CVVHF, the effluent bag turned bright pink. Given the pink color of the effluent bag and the hypothesis of propofol-induced pink urine syndrome, propofol was replaced by midazolam. After stopping propofol, the color of effluent bag lightened. Unfortunately, the patient died on the third day of hospitalization due to diffuse cerebral edema.
We report here the first case of pink urine syndrome as revealed by the change in color of the contents of the CVVHF effluent bag in an anuric patient. This syndrome is rare but significant in anesthesia/intensive care settings, where propofol is a frequently used sedative. Knowledge of this syndrome appears to be important to avoid irrelevant additional investigations and to optimize the therapeutic strategy.
粉红色尿综合征是一种罕见且尚未被充分认识的疾病,常由肥胖、胰岛素抵抗和药物异丙酚引起。其特征为粉红色尿或尿沉渣,且在无卟啉或食物源性色素的情况下出现。该综合征的病理生理学尚未完全阐明,但与尿酸代谢紊乱有关。与其他异丙酚输注并发症相比,麻醉医生对粉红色尿综合征的了解较少。我们的病例报告旨在强调这种罕见的综合征,其诊断和治疗可能具有挑战性。我们报告了首例通过连续静脉-静脉血液滤过(CVVHF)过程中流出袋颜色变化证实的该综合征。
一名 61 岁女性因室性心律失常导致心肺复苏后被收入重症监护病房。她接受了低温治疗,使用异丙酚(300mg/h)镇静,并开始进行 CVVHF 治疗,以治疗少尿型急性肾损伤伴严重代谢性酸中毒。在开始 CVVHF 几个小时后,流出袋变成鲜艳的粉红色。鉴于流出袋的粉红色以及异丙酚诱导的粉红色尿综合征的假设,异丙酚被咪达唑仑取代。停止异丙酚后,流出袋的颜色变浅。不幸的是,患者在住院第三天因弥漫性脑水肿死亡。
我们报告了首例通过无尿患者 CVVHF 流出袋内容物颜色变化揭示的粉红色尿综合征。该综合征虽罕见,但在麻醉/重症监护环境中意义重大,因为异丙酚是一种常用的镇静剂。了解该综合征似乎很重要,可避免不必要的额外检查,并优化治疗策略。