Nephrology and Dialysis Unit, Magna Graecia University, Catanzaro, Italy.
Department of Medical and Surgical Sciences-Renal Unit, University "Magna Graecia", Campus Salvatore Venuta, Viale Europa, 88100, Catanzaro, Italy.
J Nephrol. 2024 Sep;37(7):1863-1870. doi: 10.1007/s40620-024-02032-4. Epub 2024 Aug 5.
Mortality and cardiovascular (CV) risk prediction in individuals with end-stage kidney disease (ESKD) on chronic hemodialysis (HD) remains challenging due to the multitude of implicated factors. In a multicenter ESKD-HD cohort, we tested the prognostic yield of the assessment of circulating Humanin, a small mitochondrial-derived peptide involved in CV protection, on CV events and mortality.
We conducted a prospective, observational, pilot study on 94 prevalent HD patients. The prognostic capacity of circulating Humanin levels was tested on a primary composite (all-cause mortality + non-fatal CV events) and a secondary exploratory endpoint (all-cause mortality alone).
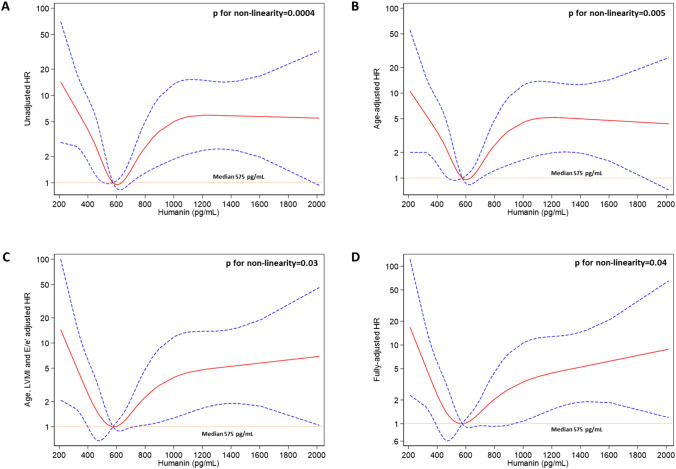
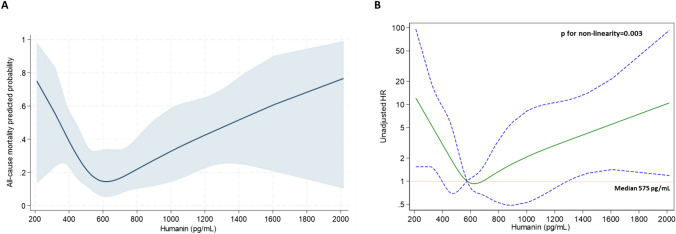
Baseline Humanin level was comparable in patients reaching the primary or secondary endpoint as compared to others (p = 0.69 and 0.76, respectively). Unadjusted followed by multivariable Cox regression analyses adjusted for age, left ventricular mass index (LVMi), E/e', pulse pressure and diabetes mellitus indicated a non-linear relationship between Humanin levels and the composite outcome with the highest Hazard Ratio (HR) associated with very low (< 450.7 pg/mL; HR ranging from 4.25 to 2.49) and very high (> 759.5 pg/mL; HR ranging from 5.84 to 4.50) Humanin values. Restricted cubic splines fitting univariate and multivariate Cox regression analyses visually confirmed a curvilinear trend with an increasing risk observed for lower and higher Humanin values around the median, respectively. A similar, u-shaped association was also evidenced with the secondary endpoint.
Altered Humanin levels may impart prognostic information in ESKD-HD patients at risk of death or CV events. Future investigations are needed to confirm whether Humanin measurement could improve CV and mortality risk prediction beyond traditional risk models.
由于涉及多种因素,终末期肾病(ESKD)患者在接受慢性血液透析(HD)治疗时的死亡率和心血管(CV)风险预测仍然具有挑战性。在一项多中心 ESKD-HD 队列研究中,我们检测了循环 Humanin 的评估对 CV 事件和死亡率的预后价值,Humanin 是一种参与 CV 保护的小型线粒体衍生肽。
我们对 94 例现患 HD 患者进行了前瞻性、观察性、试点研究。循环 Humanin 水平的预后能力在主要复合终点(全因死亡率+非致死性 CV 事件)和次要探索性终点(全因死亡率)上进行了测试。
与未达到主要或次要终点的患者相比,达到主要或次要终点的患者的基线 Humanin 水平无差异(p=0.69 和 0.76)。未调整的 Cox 回归分析和多变量 Cox 回归分析,校正年龄、左心室质量指数(LVMi)、E/e'、脉压和糖尿病,表明 Humanin 水平与复合结局之间呈非线性关系,最高的风险比(HR)与极低(<450.7 pg/mL;HR 范围为 4.25 至 2.49)和极高(>759.5 pg/mL;HR 范围为 5.84 至 4.50)Humanin 值相关。单变量和多变量 Cox 回归分析的限制性立方样条拟合直观地证实了一种曲线趋势,分别在中位数左右低值和高值时观察到风险增加。次要终点也证明了类似的 U 形关联。
改变的 Humanin 水平可能为处于死亡或 CV 事件风险中的 ESKD-HD 患者提供预后信息。需要进一步的研究来证实 Humanin 测量是否可以改善传统风险模型以外的 CV 和死亡率风险预测。