The Healthcare Innovation Center (THINC), Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
Department of Epidemiology and Health Economics, Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
PLoS One. 2024 Aug 5;19(8):e0307881. doi: 10.1371/journal.pone.0307881. eCollection 2024.
Cochlear Implant (CI) has been shown to improve speech comprehension, sound localization and tinnitus in adults with Single-Sided-Deafness (SSD) compared to standard treatment currently available in the Dutch setting such as a CROS (Contralateral Routing of Signals) hearing device or a BCD (Bone Conduction Device). Also, for the pediatric population with SSD, CI has shown to be clinically meaningful. Because currently no information is available on the health economic effects of CI in adults and children with SSD in the Netherlands, a cost-utility analysis was conducted.
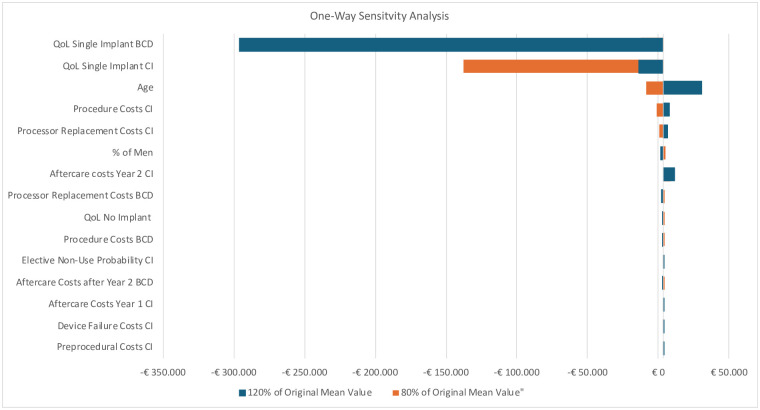
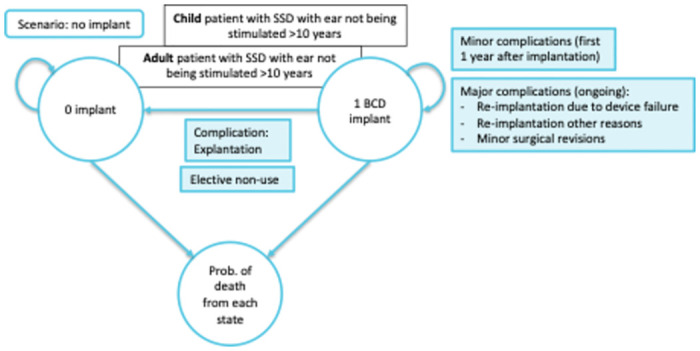
We developed a Markov cohort model, for both the adult and pediatric SSD population, with three states: implant, no implant, and dead. CI was compared with the Bone Conduction Device (BCD) treatment, requiring surgery and no specific treatment. The time horizon of the model was lifelong, costs were discounted with 3% and effects with 1.5%. A societal perspective was taken, including productivity costs in the analysis, with costing data based on publicly available prices for the Netherlands. Values for clinical outcome parameters, i.e. hearing gain, and event probabilities were based on existing literature. Deterministic and probabilistic sensitivity analyses as well as scenario analyses were performed to outline uncertainty of individual and combined parameters.
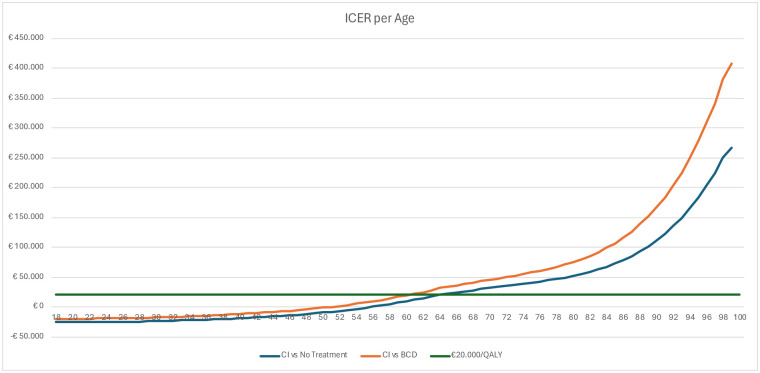
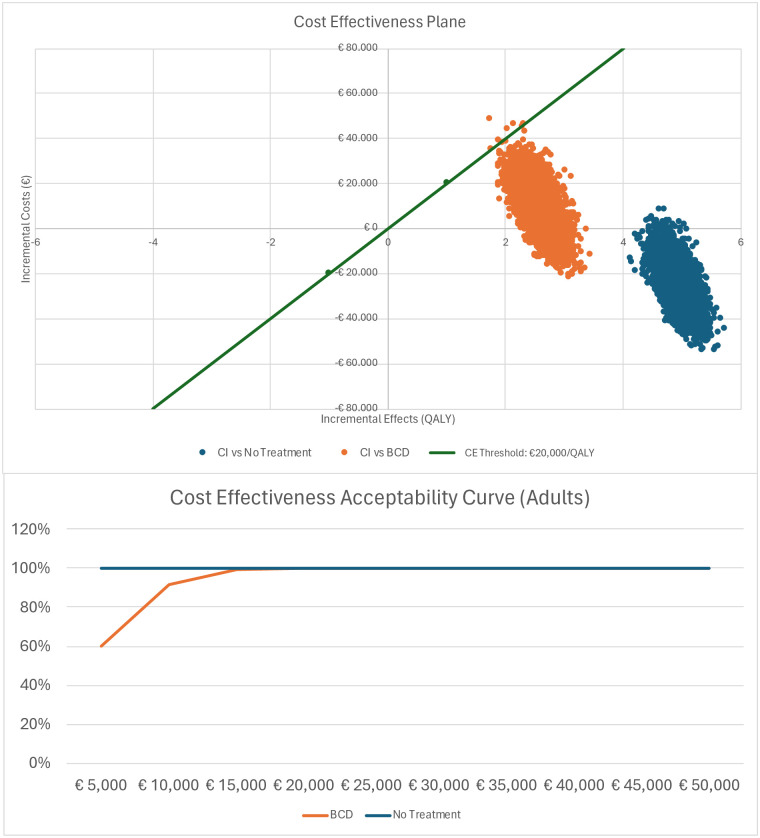
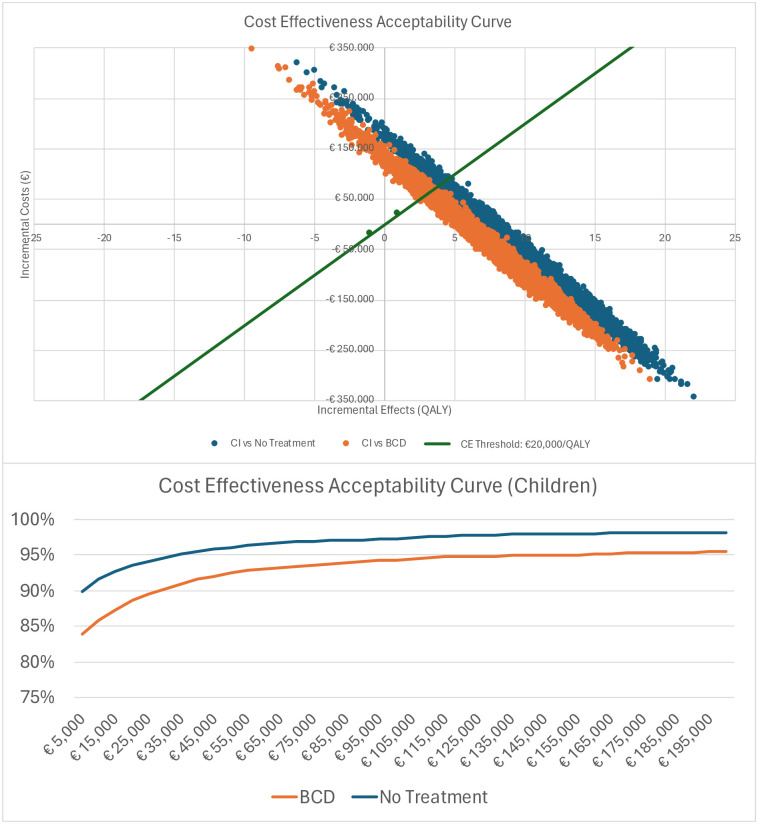
Mean per patient costs for CI in the adult population were €194,051 (95%-CrI €177,274 to €211,108) compared to the total costs of €185,310 (95%-CrI €182,367 to €194,142) for BCD resulting in a cost difference of €8,826 (95%-CrI -€5,020 to €18,252). Compared to no treatment, the cost difference was -€25,089 (95%-CrI -€31,678 to -€6,003). Adults who were treated with CI gained 18.41 (95%-CrI 18.07 to 18.75) quality adjusted life years (QALY) whereas BCD patients gained 15.81 QALYs (95%-CrI 15.53 to 16.10), a difference of 2.60 QALYs (95%-CrI 2.15 to 3.05). The Incremental Cost Effectiveness Ratio (ICER) for adults with CI was determined to be €3,494/QALY gained. Patient without treatment gained 13.46 QALY (95%-CrI 13.20 to 13.73), a difference of 4.95 (95%-CrI 4.87 to 5.01) resulting in CI dominating no treatment. The ICER remained below the Dutch threshold of €20,000/QALY. The probabilistic sensitivity analyses confirmed the results. For children, CI dominated when compared to BCD and when compared to no treatment. Compared to BCD, CI led to a cost saving of €29,611 (95%-CrI -€126,800 to €54,375) and compared to no treatment, CI resulted in a cost saving of €57,658 (95%-CrI -€146,687 to €5,919). The incremental QALY gain compared to BCD was 7.22 (95%-CrI 4.19 to 8.55) and 26.03 (95%-CrI 20.82 to 31.06) compared to no treatment.
Based on the results of this health economic evaluation with a Markov cohort model, it is very likely that CI is cost-effective compared to BCD and to no treatment in the Dutch adult and pediatric population with SSD. In both populations the ICER was below the Dutch cost-effectiveness threshold of €20,000/QALY.
与目前荷兰标准治疗方法(如 CROS(对侧信号转导)听力设备或 BCD(骨导设备)相比,人工耳蜗植入 (CI) 已被证明可提高单侧聋 (SSD) 成人的言语理解、声源定位和耳鸣。此外,对于 SSD 的儿科人群,CI 已被证明具有临床意义。由于目前尚无关于荷兰 SSD 成人和儿童 CI 的健康经济学影响的信息,因此进行了成本效用分析。
我们为 SSD 的成人和儿科人群开发了一个马尔可夫队列模型,有三个状态:植入、未植入和死亡。CI 与骨导设备 (BCD) 治疗进行比较,后者需要手术且无特定治疗。模型的时间范围是终身的,成本贴现率为 3%,效果贴现率为 1.5%。采用社会视角,包括分析中的生产力成本,基于荷兰公开价格的成本数据。临床结果参数(即听力增益和事件概率)的值基于现有文献。进行了确定性和概率敏感性分析以及情景分析,以概述个体和组合参数的不确定性。
成人人群中 CI 的平均每位患者成本为 194,051 欧元(95%-CrI 为 177,274 至 211,108 欧元),而 BCD 的总费用为 185,310 欧元(95%-CrI 为 182,367 至 194,142 欧元),因此成本差异为 8,826 欧元(95%-CrI 为-5,020 至 18,252 欧元)。与无治疗相比,成本差异为-25,089 欧元(95%-CrI 为-31,678 至-6,003 欧元)。接受 CI 治疗的成年人获得了 18.41(95%-CrI 为 18.07 至 18.75)个质量调整生命年 (QALY),而 BCD 患者获得了 15.81 QALY(95%-CrI 为 15.53 至 16.10),差异为 2.60 QALY(95%-CrI 为 2.15 至 3.05)。成人 CI 的增量成本效益比 (ICER) 确定为 3494 欧元/QALY。无治疗的患者获得了 13.46 QALY(95%-CrI 为 13.20 至 13.73),差异为 4.95(95%-CrI 为 4.87 至 5.01),导致 CI 优于无治疗。ICER 仍低于荷兰 20,000 欧元/QALY 的阈值。概率敏感性分析证实了结果。对于儿童,CI 与 BCD 和无治疗相比具有优势。与 BCD 相比,CI 可节省 29,611 欧元(95%-CrI 为-126,800 至 54,375 欧元),与无治疗相比,CI 可节省 57,658 欧元(95%-CrI 为-146,687 至 5,919 欧元)。与 BCD 相比,CI 的增量 QALY 增益为 7.22(95%-CrI 为 4.19 至 8.55),与无治疗相比为 26.03(95%-CrI 为 20.82 至 31.06)。
基于这项使用马尔可夫队列模型的健康经济学评估的结果,CI 很可能在荷兰 SSD 成人和儿科人群中具有成本效益,与 BCD 和无治疗相比。在这两个人群中,ICER 均低于荷兰 20,000 欧元/QALY 的成本效益阈值。