Suhagiya Gaurang H, Hamid Insha H, Agago Demeke E, Arsalan Muhammad, Dhakecha Mayankkumar D, Chaudhari Sandipkumar S, Wei Calvin R, Ali Neelum
Medicine, Jiangsu University, Zhenjiang, CHN.
Physiology, Government Medical College (GMC) Srinagar, Srinagar, IND.
Cureus. 2024 Jul 4;16(7):e63795. doi: 10.7759/cureus.63795. eCollection 2024 Jul.
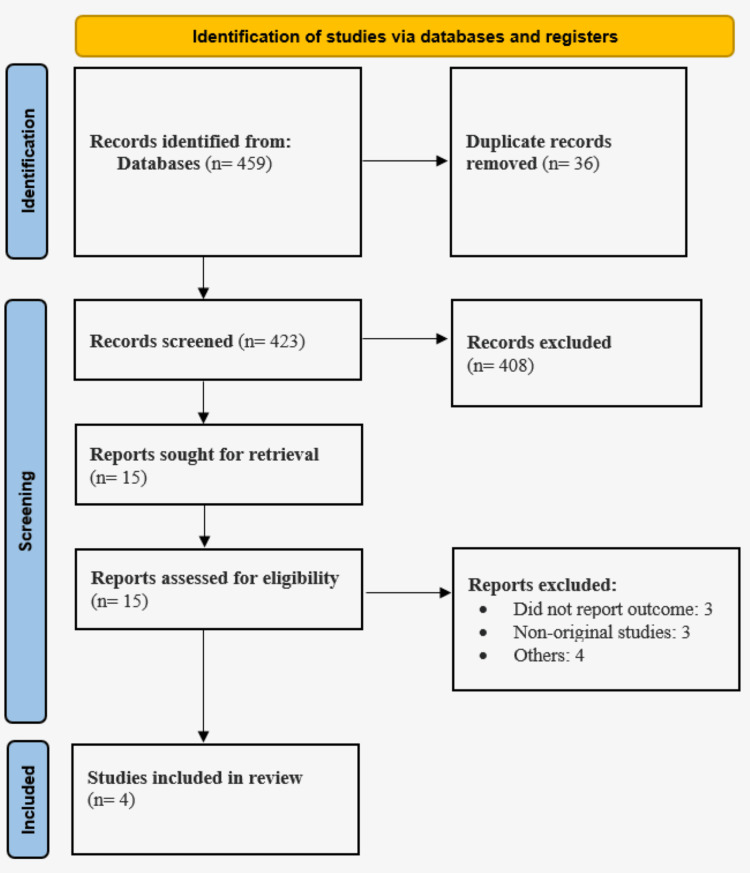
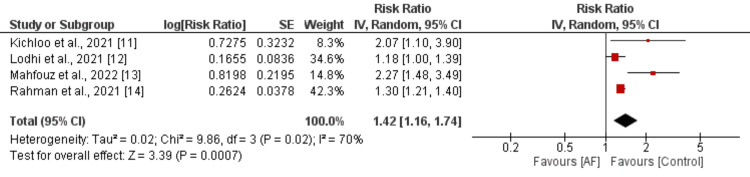
Inflammatory bowel disease (IBD) is a chronic inflammatory condition affecting the gastrointestinal tract, often leading to symptoms like abdominal pain and diarrhea. Given the increasing evidence linking systemic inflammation to atrial fibrillation development, investigating IBD as a potential risk factor for atrial fibrillation becomes imperative. This meta-analysis aims to evaluate the impact of atrial fibrillation on inpatient outcomes, resource utilization, and length of hospital stays among IBD patients. Following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 guidelines, a systematic literature search was conducted across multiple databases, including Embase, PubMed, Scopus, and Web of Science, from the inception of databases to June 5, 2024. Eligible studies included prospective or retrospective studies with definitive diagnoses of ulcerative colitis, Crohn's disease, or IBD, demonstrating the influence of atrial fibrillation. Data were extracted, and quality assessment was performed using the Newcastle-Ottawa Scale. The meta-analysis comprised 842,149 IBD patients, with 71,221 having atrial fibrillation. Pooled analysis revealed a significant association between atrial fibrillation and heightened all-cause mortality risk (risk ratio (RR): 1.42, 95% confidence interval (CI): 1.16 to 1.74, p<0.01). However, no significant differences were observed in the incidence of acute myocardial infarction, acute kidney injury, or acute respiratory failure between patients with and without atrial fibrillation. IBD patients with comorbid atrial fibrillation face higher mortality rates, potentially due to systemic inflammation, thromboembolism risks, polypharmacy, and the complexities of managing both conditions concurrently. Early identification and integrated management of atrial fibrillation in IBD patients are crucial to improving outcomes. Larger, multi-center studies are needed to explore the underlying mechanisms and develop tailored treatment strategies.
炎症性肠病(IBD)是一种影响胃肠道的慢性炎症性疾病,常导致腹痛和腹泻等症状。鉴于越来越多的证据表明全身性炎症与心房颤动的发生有关,因此有必要将IBD作为心房颤动的潜在危险因素进行研究。本荟萃分析旨在评估心房颤动对IBD患者住院结局、资源利用和住院时间的影响。按照系统评价和荟萃分析的首选报告项目(PRISMA)2020指南,从数据库建立至2024年6月5日,在多个数据库(包括Embase、PubMed、Scopus和Web of Science)中进行了系统的文献检索。符合条件的研究包括对溃疡性结肠炎、克罗恩病或IBD进行明确诊断的前瞻性或回顾性研究,以证明心房颤动的影响。提取数据,并使用纽卡斯尔-渥太华量表进行质量评估。该荟萃分析纳入了842149例IBD患者,其中71221例患有心房颤动。汇总分析显示,心房颤动与全因死亡风险升高之间存在显著关联(风险比(RR):1.42,95%置信区间(CI):1.16至1.74,p<0.01)。然而,在有心房颤动和无心房颤动的患者之间,急性心肌梗死、急性肾损伤或急性呼吸衰竭的发生率没有显著差异。合并心房颤动的IBD患者面临更高的死亡率,这可能是由于全身性炎症、血栓栓塞风险、联合用药以及同时管理这两种疾病的复杂性所致。早期识别和综合管理IBD患者的心房颤动对于改善结局至关重要。需要开展更大规模的多中心研究,以探索潜在机制并制定针对性的治疗策略。