Al-Azizi Karim, Shih Emily, DiMaio J Michael, Squiers John J, Moubarak Ghadi, Kluis Austin, Banwait Jasjit K, Ryan William H, Szerlip Molly I, Potluri Srinivasa P, Hamandi Mohanad, Lanfear Allison T, Meidan Talia G, Stoler Robert C, Mixon Timothy A, Krueger Anita R, Mack Michael J
Department of Cardiology, Baylor Scott & White The Heart Hospital, Plano, Texas.
Department of Cardiothoracic Surgery, Baylor Scott & White The Heart Hospital, Plano, Texas.
J Soc Cardiovasc Angiogr Interv. 2023 Apr 21;2(3):100600. doi: 10.1016/j.jscai.2023.100600. eCollection 2023 May-Jun.
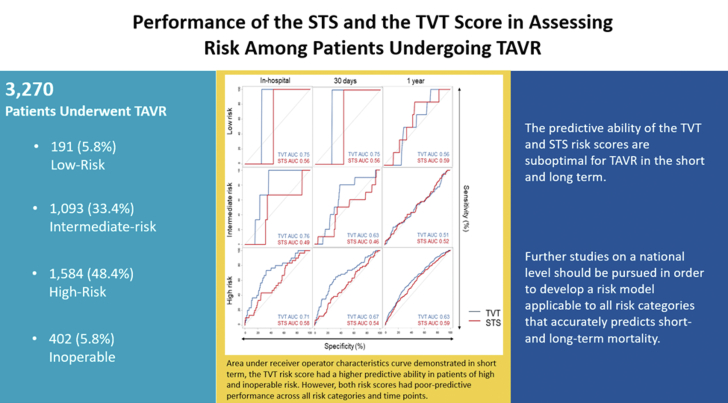
The Society of Thoracic Surgeons (STS) score has been used to risk stratify patients undergoing transcatheter aortic valve replacement (TAVR). The Transcatheter Valve Therapy (TVT) score was developed to predict in-hospital mortality in high/prohibitive-risk patients. Its performance in low and intermediate-risk patients is unknown. We sought to compare TVT and STS scores' ability to predict clinical outcomes in all-surgical-risk patients undergoing TAVR.
Consecutive patients undergoing TAVR from 2012-2020 within a large health care system were retrospectively reviewed and stratified by STS risk score. Predictive abilities of TVT and STS scores were compared using observed-to-expected mortality ratios (O:E) and area under the receiver operating characteristics curves (AUCs) for 30-day and 1-year mortality.
We assessed a total of 3270 patients (mean age 79 ± 9 years, 45% female), including 191 (5.8%) low-risk, 1093 (33.4%) intermediate-risk, 1584 (48.4%) high-risk, and 402 (5.8%) inoperable. Mean TVT and STS scores were 3.5% ± 2.0% and 6.1% ± 4.3%, respectively. Observed 30-day and 1-year mortality were 2.8% (92/3270; O:E TVT 0.8 ± 0.16 vs STS 0.46 ± 0.09), and 13.2% (432/3270), respectively. In the all-comers population, both TVT and STS risk scores showed poor prediction of 30-day (AUC: TVT 0.68 [0.62-0.74] vs STS 0.64 [0.58-0.70]), and 1-year (AUC: TVT 0.65 [0.62-0.58] vs STS 0.65 [0.62-0.58]) mortality. After stratifying by surgical risk, discrimination of the TVT and STS scores remained poor in all categories at 30 days and 1 year.
An updated TAVR risk score with improved predictive ability across all-surgical-risk categories should be developed based on a larger national registry.
胸外科医师协会(STS)评分已用于对接受经导管主动脉瓣置换术(TAVR)的患者进行风险分层。经导管瓣膜治疗(TVT)评分旨在预测高风险/极高风险患者的住院死亡率。其在低风险和中风险患者中的表现尚不清楚。我们试图比较TVT和STS评分在接受TAVR的所有手术风险患者中预测临床结局的能力。
对2012年至2020年在一个大型医疗保健系统中接受TAVR的连续患者进行回顾性研究,并根据STS风险评分进行分层。使用观察到的与预期的死亡率之比(O:E)以及30天和1年死亡率的受试者工作特征曲线下面积(AUC)比较TVT和STS评分的预测能力。
我们共评估了3270例患者(平均年龄79±9岁,45%为女性),包括191例(5.8%)低风险、1093例(33.4%)中风险、1584例(48.4%)高风险和402例(5.8%)无法手术的患者。TVT和STS评分的平均值分别为3.5%±2.0%和6.1%±4.3%。观察到的30天和1年死亡率分别为2.8%(92/3270;TVT的O:E为0.8±0.16,STS为0.46±0.09)和13.2%(432/3270)。在所有患者群体中,TVT和STS风险评分对30天(AUC:TVT为0.68[0.62 - 0.74],STS为0.64[0.58 - 0.70])和1年(AUC:TVT为0.65[0.62 - 0.58],STS为0.65[0.62 - 0.58])死亡率的预测均较差。按手术风险分层后,TVT和STS评分在30天和1年时在所有类别中的区分能力仍然较差。
应基于更大规模的全国性登记数据开发一种在所有手术风险类别中具有更高预测能力的更新TAVR风险评分。