Kadantseva Kristina, Subbotin Valery, Akchulpanov Roman, Berikashvili Levan, Yadgarov Mikhail, Zhukova Lyudmila, Kvetenadze Guram, Svitich Oxana, Kukina Polina, Kuznetsov Ivan, Shemetova Mariya, Smirnova Anastasiya, Polyakov Petr, Shebankov Andrey, Likhvantsev Valery
Department of Clinical Trials and intelligent IT, Federal Research and Clinical Centre of Intensive Care Medicine and Rehabilitology, Moscow, Russia.
Department of Intensive Care and Anesthesiology, A. Loginov Moscow Clinical Scientific Center, Moscow, Russia.
Front Oncol. 2024 Jul 26;14:1401910. doi: 10.3389/fonc.2024.1401910. eCollection 2024.
Breast cancer (BC) mortality primarily stems from metastases rather than the primary tumor itself. Perioperative stress, encompassing both surgical and anesthetic factors, profoundly impacts the immune system, leading to alterations in neuroendocrine pathways and immune functions, potentially facilitating tumor progression and metastasis. Understanding the immunomodulatory effects of different anesthesia techniques is crucial for optimizing perioperative care in patients with BC. The neutrophil-to-lymphocyte ratio (NLR) serves as one of the key indicators of perioperative immune response.
To compare the effects of inhalation anesthesia (IA) and total intravenous anesthesia (TIVA) on perioperative immune response in BC surgery patients.
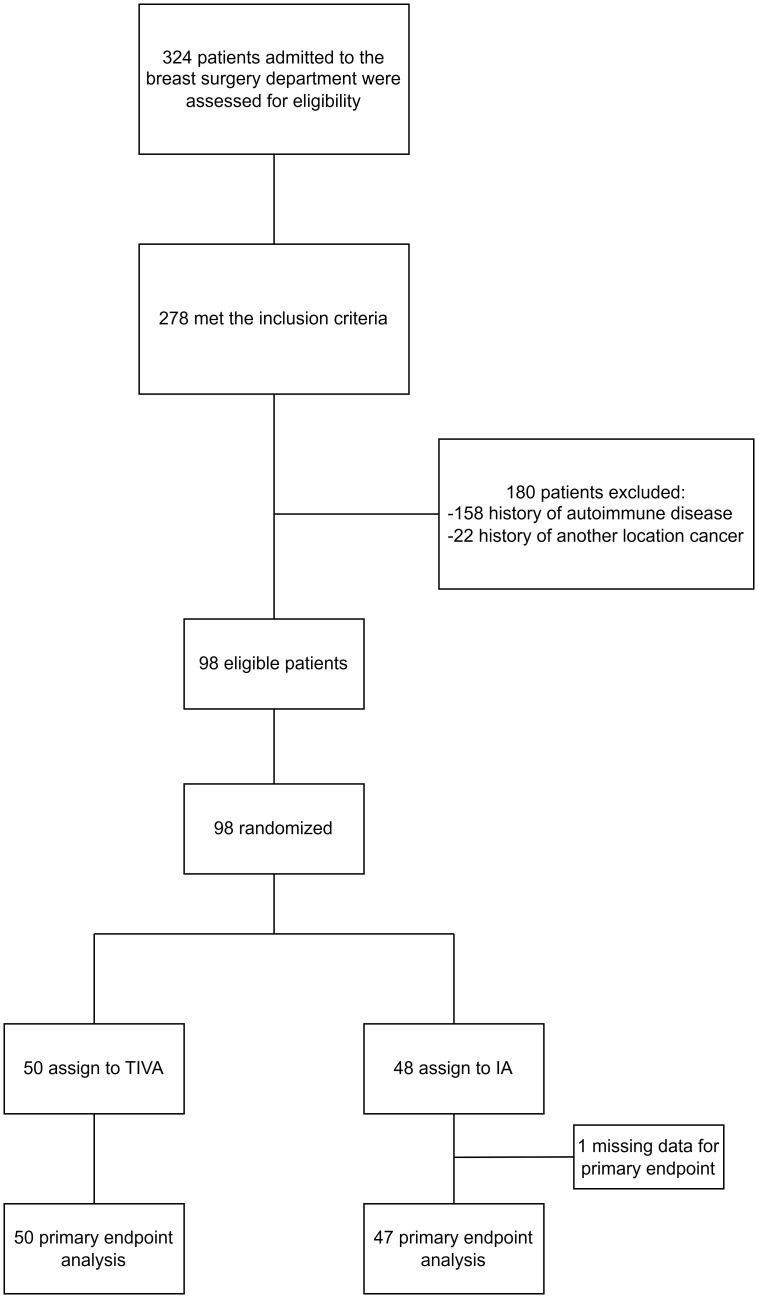
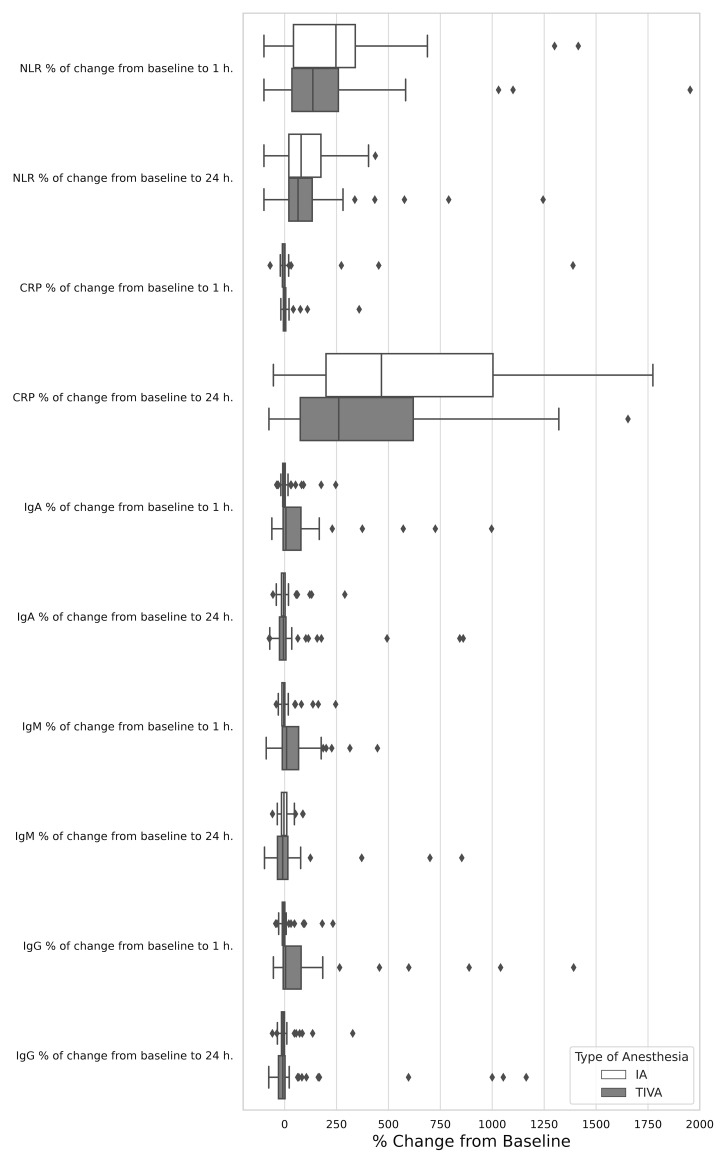
In this randomized, double-blind clinical trial, BC surgery patients were randomized to receive either TIVA with propofol or IA with sevoflurane. The primary endpoint was NLR assessment. Secondary immune parameters measured included natural killer cells, various T cell subsets, B cells, the immuno-regulatory index [T-helpers (CD3+CD4+)/cytotoxic T-cells (CD3+CD8+)], matrix metallopeptidases (MMP-9), complement components, and immunoglobulins, preoperatively and at 1 and 24 hours postoperatively.
The study included 98 patients (IA: 48, TIVA: 50). The baseline characteristics exhibited remarkable similarity across the groups. No significant difference in absolute NLR values was found between IA and TIVA groups at any time point (1 hour: p = 0.519, 24 hours: p = 0.333). Decreased IgA and IgM levels post-surgery suggested potential negative impacts of IA on humoral immunity compared to TIVA. CRP levels increased more by 24 hours (p = 0.044) in IA compared to TIVA. No significant differences were observed in natural killer cells, T cell subsets, B cells, MMP-9 levels or complement components between groups. Significant differences in the immuno-regulatory index between the TIVA and IA groups at one hour postoperatively (p = 0.033) were not maintained at 24 hours.
While there were no notable differences in NLR among the types of anesthesia, the observed disparities in immunoglobulin content and C-reactive protein levels between groups suggest that we cannot dismiss the potential immunosuppressive effects of inhalational anesthesia in breast cancer surgeries. Further investigation needed to clarify the impact of various anesthesia methods on immune function and their implications for long-term cancer outcomes.
乳腺癌(BC)死亡率主要源于转移,而非原发肿瘤本身。围手术期应激,包括手术和麻醉因素,会深刻影响免疫系统,导致神经内分泌途径和免疫功能改变,可能促进肿瘤进展和转移。了解不同麻醉技术的免疫调节作用对于优化BC患者的围手术期护理至关重要。中性粒细胞与淋巴细胞比值(NLR)是围手术期免疫反应的关键指标之一。
比较吸入麻醉(IA)和全静脉麻醉(TIVA)对BC手术患者围手术期免疫反应的影响。
在这项随机、双盲临床试验中,BC手术患者被随机分为接受丙泊酚TIVA或七氟醚IA。主要终点是NLR评估。测量的次要免疫参数包括自然杀伤细胞、各种T细胞亚群、B细胞、免疫调节指数[T辅助细胞(CD3 + CD4 +)/细胞毒性T细胞(CD3 + CD8 +)]、基质金属蛋白酶(MMP - 9)、补体成分和免疫球蛋白,在术前以及术后1小时和24小时进行测量。
该研究纳入了98例患者(IA组:48例,TIVA组:50例)。各组间基线特征表现出显著相似性。IA组和TIVA组在任何时间点的绝对NLR值均无显著差异(1小时:p = 0.519,24小时:p = 0.333)。与TIVA相比,术后IgA和IgM水平降低表明IA对体液免疫可能有负面影响。与TIVA相比,IA组术后24小时CRP水平升高幅度更大(p = 0.044)。各组间自然杀伤细胞、T细胞亚群、B细胞、MMP - 9水平或补体成分均未观察到显著差异。术后1小时TIVA组和IA组免疫调节指数的显著差异(p = 0.033)在24小时时未持续存在。
虽然不同类型麻醉之间NLR无显著差异,但各组间观察到的免疫球蛋白含量和C反应蛋白水平差异表明,我们不能忽视吸入麻醉在乳腺癌手术中的潜在免疫抑制作用。需要进一步研究以阐明各种麻醉方法对免疫功能的影响及其对长期癌症结局的意义。