Papakonstantinou Menelaos, Fiflis Stylianos, Giakoustidis Alexandros, Christodoulidis Grigorios, Myriskou Athanasia, Louri Eleni, Papalavrentios Lavrentios, Papadopoulos Vasileios N, Giakoustidis Dimitrios
A' Department of Surgery, General Hospital Papageorgiou, School of Medicine, Faculty of Medical Sciences, Aristotle University of Thessaloniki, Thessaloniki, Greece.
Department of General Surgery, University Hospital of Larissa, Larissa, Greece.
Ann Hepatobiliary Pancreat Surg. 2024 Nov 30;28(4):423-432. doi: 10.14701/ahbps.24-118. Epub 2024 Aug 14.
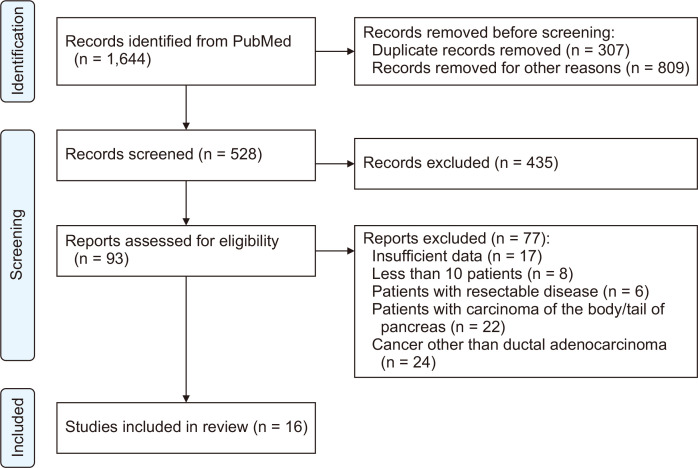
Pancreatic ductal adenocarcinoma (PDAC) is one of the most aggressive tumors, and the most common cause of cancer-related deaths. In the past, vascular infiltration of the tumor rendered the disease unresectable. However, today, venous or arterial involvement of a PDAC is classified as borderline resectable (BR) or locally advanced (LA) disease. Pancreaticoduodenectomy (PD) with vascular resections is a promising intervention intended for complete resection of BR- and LA-PDAC. This study aims to assess the overall survival of patients undergoing PD with vascular resections, compared to those without. A PubMed search was conducted for cohort studies that included patients with BR- or LA-PDAC treated with vascular resections. The retrieved publications were screened following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist. The study protocol was registered at the International Prospective Register for Systematic Reviews (PROSPERO). Sixteen cohort studies were included in our systematic review. Fourteen of them included patients undergoing PD with venous-only resections for PDAC. The 5-year overall survival rates ranged from 8.0% to 22.2% for vascular resection patients, and 4.0% to 24.3% for standard PD patients. Three cohorts included patients with PDAC and arterial and/or venous involvement who were treated with arterial resections. Their median overall survival ranged from 13.7 to 17.0 months, similar to that of patients who did not undergo vascular resections. PD with vascular resections in patients with BR- and LA-PDAC could lead to similar overall survival to that after standard PD.
胰腺导管腺癌(PDAC)是侵袭性最强的肿瘤之一,也是癌症相关死亡的最常见原因。过去,肿瘤的血管浸润使该疾病无法切除。然而,如今,PDAC的静脉或动脉受累被归类为可切除边缘(BR)或局部晚期(LA)疾病。血管切除的胰十二指肠切除术(PD)是一种有前景的干预措施,旨在完全切除BR和LA-PDAC。本研究旨在评估接受血管切除的PD患者与未接受血管切除的患者的总生存期。在PubMed上搜索了队列研究,这些研究纳入了接受血管切除治疗的BR或LA-PDAC患者。根据系统评价和Meta分析优先报告条目(PRISMA)清单对检索到的出版物进行筛选。该研究方案已在国际前瞻性系统评价注册库(PROSPERO)注册。我们的系统评价纳入了16项队列研究。其中14项纳入了仅接受PDAC静脉切除的PD患者。血管切除患者的5年总生存率为8.0%至22.2%,标准PD患者为4.0%至24.3%。三项队列纳入了患有PDAC且有动脉和/或静脉受累并接受动脉切除治疗的患者。他们的中位总生存期为13.7至17.0个月,与未接受血管切除的患者相似。BR和LA-PDAC患者进行血管切除的PD可能导致与标准PD相似的总生存期。