Onishi Tatsuki
Data Science and AI Innovation Research Promotion Center, Shiga University, 1 Chome-1-1 Bamba, Hikone, Shiga, 522-0069, Japan, 81 749 27 1030.
Department of Anesthesia, Juntendo University Shizuoka Hospital, Izunokuni, Shizuoka, Japan.
JMIRx Med. 2024 Aug 14;5:e56405. doi: 10.2196/56405.
Sleeve gastrectomy is an effective surgical option for morbid obesity, and it improves glucose homeostasis. In patients with gastric cancer and type 2 diabetes mellitus (DM), gastrectomy, including total gastrectomy, is beneficial for glycemic control.
This study aims to clarify the effects of gastrectomy and different reconstructive techniques on the incidence of postoperative DM in patients with gastric cancer.
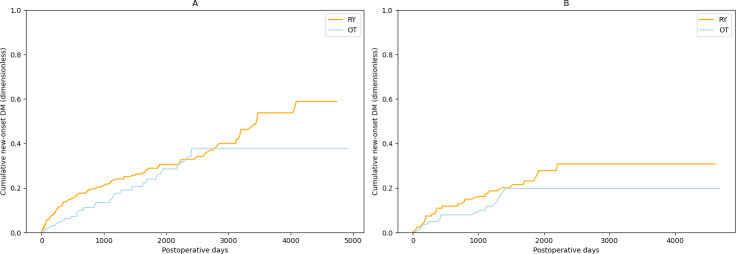
This retrospective, single-center, cohort study included 715 patients without DM who underwent total gastrectomy at the Tokyo Metropolitan Bokutoh Hospital between August 2005 and March 2019. Patients underwent reconstruction by Roux-en-Y (RY) gastric bypass or other surgical techniques (OT), with DM onset determined by hemoglobin A1c levels or medical records. Analyses included 2-sample, 2-tailed t tests; χ2 tests; and the Kaplan-Meier method with log-rank tests to compare the onset curves between the RY and OT groups, along with additional curves stratified by sex. A Swimmer plot for censoring and new-onset DM was implemented.
Stratified data analysis compared the RY and OT reconstruction methods. The hazard ratio was 1.52 (95% CI 1.06-2.18; P=.02), which indicated a statistically significant difference in the incidence of new-onset diabetes between the RY and OT groups in patients with gastric cancer. The hazard ratio after propensity score matching was 1.42 (95% CI 1.09-1.86; P=.009).
This first-of-its-kind study provides insight into how different methods of gastric reconstruction affect postoperative diabetes. The results suggest significant differences in new-onset DM after surgery based on the reconstruction method. This research highlights the need for careful surgical planning to consider potential postoperative DM, particularly in patients with a family history of DM. Future studies should investigate the role of gut microbiota and other reconstructive techniques, such as laparoscopic jejunal interposition, in developing postoperative DM.
袖状胃切除术是治疗病态肥胖的一种有效手术方式,且能改善葡萄糖稳态。在胃癌合并2型糖尿病(DM)患者中,包括全胃切除术在内的胃切除术对血糖控制有益。
本研究旨在阐明胃切除术及不同重建技术对胃癌患者术后DM发生率的影响。
这项回顾性、单中心队列研究纳入了2005年8月至2019年3月期间在东京都墨东医院接受全胃切除术的715例无DM患者。患者接受了Roux-en-Y(RY)胃旁路术或其他手术技术(OT)进行重建,DM发病通过糖化血红蛋白水平或病历确定。分析包括双样本、双尾t检验;χ2检验;以及采用对数秩检验的Kaplan-Meier方法,以比较RY组和OT组之间的发病曲线,以及按性别分层的其他曲线。实施了用于审查和新发DM的游泳者图。
分层数据分析比较了RY和OT重建方法。风险比为1.52(95%CI 1.06-2.18;P=0.02),这表明胃癌患者中RY组和OT组新发糖尿病的发生率存在统计学显著差异。倾向得分匹配后的风险比为1.42(95%CI 1.09-1.86;P=0.009)。
这项同类研究中的首例研究深入探讨了不同的胃重建方法如何影响术后糖尿病。结果表明,基于重建方法,术后新发DM存在显著差异。本研究强调了在手术规划时需谨慎考虑潜在的术后DM,尤其是有DM家族史的患者。未来的研究应调查肠道微生物群和其他重建技术,如腹腔镜空肠间置术,在术后DM发生中的作用。