Arslan Murat, Schaap Jeroen, van Gorsel Bart, Aubanell Anton, Budde Ricardo P J, Hirsch Alexander, Smulders Martijn W, Mihl Casper, Damman Peter, Sliwicka Olga, Habets Jesse, Dubois Eric A, Dedic Admir
Department of Cardiology, Erasmus Medical Centre, University Medical Centre Rotterdam, Rotterdam, The Netherlands.
Department of Radiology and Nuclear Medicine, Erasmus Medical Centre, University Medical Centre Rotterdam, Rotterdam, The Netherlands.
Eur Radiol. 2025 Feb;35(2):789-797. doi: 10.1007/s00330-024-10930-1. Epub 2024 Aug 16.
To determine whether coronary computed tomography angiography (CCTA) can improve the diagnostic work-up of patients with acute chest pain and inconclusively high-sensitivity troponins (hs-troponin).
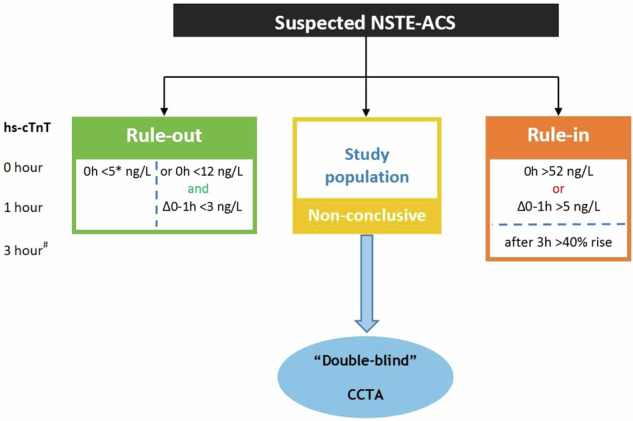
We conducted a prospective, blinded, observational, multicentre study. Patients aged 30-80 years presenting to the emergency department with acute chest pain and inconclusively elevated hs-troponins were included and underwent CCTA. The primary outcome was the diagnostic accuracy of ≥ 50% stenosis on CCTA to identify patients with type-1 non-ST-segment elevation acute coronary syndrome (NSTE-ACS).
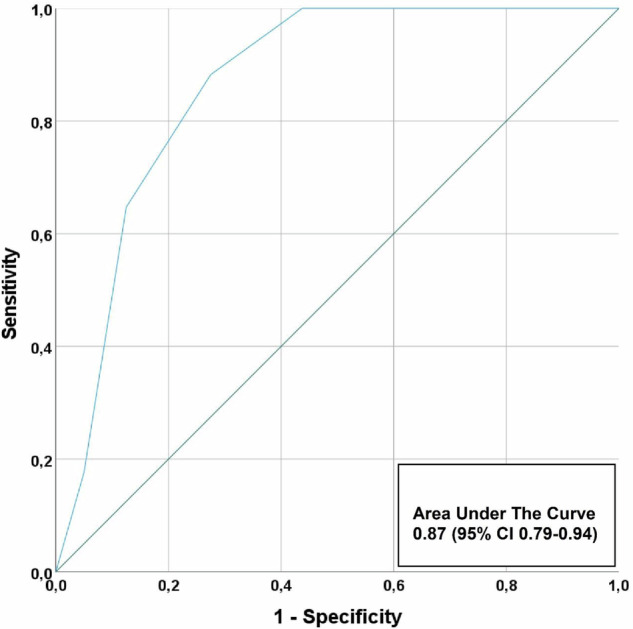
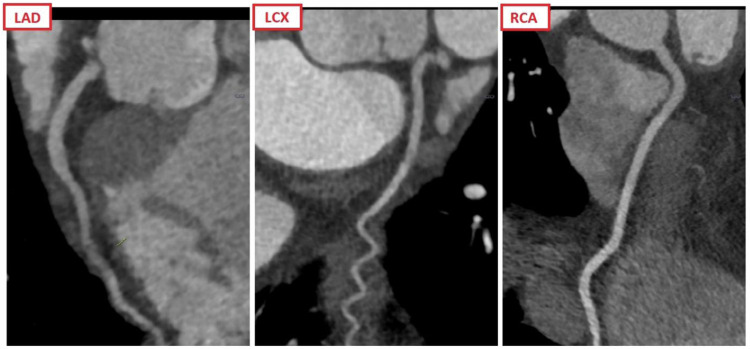
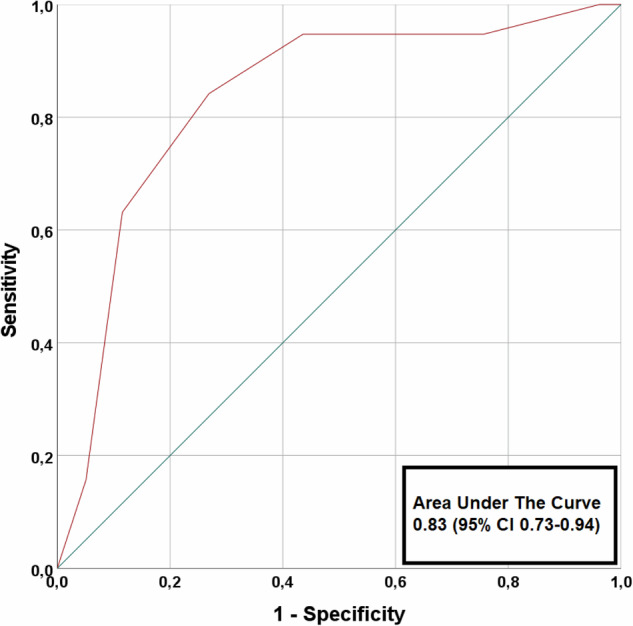
A total of 106 patients (mean age 65 ± 10, 29% women) were enrolled of whom 20 patients (19%) had an adjudicated diagnosis of type-1 NSTE-ACS. In 45 patients, CCTA revealed non-obstructive coronary artery disease (CAD) or no CAD. Sensitivity, specificity, negative predictive value (NPV), positive predictive value and area-under-the-curve (AUC) of ≥ 50% stenosis on CCTA to identify patients with type 1 NSTE-ACS, was 95% (95% confidence interval: 74-100), 56% (45-68), 98% (87-100), 35% (29-41) and 0.83 (0.73-0.94), respectively. When only coronary segments with a diameter ≥ 2 mm were considered for the adjudication of type 1 NSTE-ACS, the sensitivity and NPV increased to 100%. In 8 patients, CCTA enabled the detection of clinically relevant non-coronary findings.
The absence of ≥ 50% coronary artery stenosis on CCTA can be used to rule out type 1 NSTE-ACS in acute chest pain patients with inconclusively elevated hs-troponins. Additionally, CCTA can help improve the diagnostic work-up by detecting other relevant conditions that cause acute chest pain and inconclusively elevated hs-troponins.
Coronary CTA (CCTA) can safely rule out type 1 non-ST-segment elevation acute coronary syndrome (NSTE-ACS) in patients presenting to the ED with acute chest pain and inconclusively elevated hs-troponins, while also detecting other relevant non-coronary conditions.
Clinicaltrials.gov (NCT03129659). Registered on 26 April 2017 KEY POINTS: Acute chest discomfort is a common presenting complaint in the emergency department. CCTA achieved very high negative predictive values for type 1 NSTE-ACS in this population. CCTA can serve as an adjunct for evaluating equivocal ACS and evaluates for other pathology.
确定冠状动脉计算机断层扫描血管造影(CCTA)能否改善急性胸痛且高敏肌钙蛋白(hs - 肌钙蛋白)结果不明确患者的诊断检查。
我们开展了一项前瞻性、盲法、观察性、多中心研究。纳入年龄在30 - 80岁、因急性胸痛到急诊科就诊且hs - 肌钙蛋白升高但结果不明确的患者,并进行CCTA检查。主要结局是CCTA上≥50%狭窄对识别1型非ST段抬高型急性冠状动脉综合征(NSTE - ACS)患者的诊断准确性。
共纳入106例患者(平均年龄65±10岁,29%为女性),其中20例患者(19%)经判定诊断为1型NSTE - ACS。45例患者的CCTA显示非阻塞性冠状动脉疾病(CAD)或无CAD。CCTA上≥50%狭窄对识别1型NSTE - ACS患者的敏感性、特异性、阴性预测值(NPV)、阳性预测值和曲线下面积(AUC)分别为95%(95%置信区间:74 - 100)、56%(45 - 68)、98%(87 - 100)、35%(29 - 41)和0.83(0.73 - 0.94)。当仅考虑直径≥2mm的冠状动脉节段来判定1型NSTE - ACS时,敏感性和NPV增至100%。8例患者中,CCTA能够检测到临床相关的非冠状动脉病变。
CCTA上无≥50%冠状动脉狭窄可用于排除hs - 肌钙蛋白升高但结果不明确的急性胸痛患者的1型NSTE - ACS。此外,CCTA可通过检测导致急性胸痛和hs - 肌钙蛋白升高但结果不明确的其他相关疾病,帮助改善诊断检查。
冠状动脉CT血管造影(CCTA)可安全地排除因急性胸痛到急诊科就诊且hs - 肌钙蛋白升高但结果不明确患者的1型非ST段抬高型急性冠状动脉综合征(NSTE - ACS),同时还能检测其他相关的非冠状动脉疾病。
Clinicaltrials.gov(NCT03129659)。于2017年4月26日注册 关键点:急性胸痛是急诊科常见的就诊主诉。CCTA在该人群中对1型NSTE - ACS具有非常高的阴性预测值。CCTA可作为评估可疑ACS的辅助手段,并评估其他病变。