Pursnani Amit, Lee Ashley M, Mayrhofer Thomas, Ahmed Waleed, Uthamalingam Shanmugam, Ferencik Maros, Puchner Stefan B, Bamberg Fabian, Schlett Christopher L, Udelson James, Hoffmann Udo, Ghoshhajra Brian B
From the Cardiovascular Division, NorthShore University HealthSystem, Evanston, IL (A.P.); Cardiac MR PET CT Program, Division of Cardiology, Department of Radiology, Massachusetts General Hospital and Harvard Medical School, Boston (A.P., A.M.L., T.M., W.A., S.U., M.F., S.B.P., U.H., B.B.G.); Department of Clinical Radiology, Ludwig-Maximilians University, Klinikum Grosshadern, Munich, Germany (F.B.); Department of Diagnostic and Interventional Radiology, University Hospital Heidelberg, Heidelberg, Germany (C.L.S.); and Division of Cardiology and Cardiovascular Center, Tufts Medical Center, Boston, MA (J.U.).
Circ Cardiovasc Imaging. 2015 Mar;8(3):e002404. doi: 10.1161/CIRCIMAGING.114.002404.
Acute rest single-photon emission computed tomography-myocardial perfusion imaging (SPECT-MPI) has high predictive value for acute coronary syndrome (ACS) in emergency department patients. Prior studies have shown excellent agreement between rest/stress computed tomography perfusion (CTP) and SPECT-MPI, but the value of resting CTP (rCTP) in acute chest pain triage remains unclear. We sought to determine the diagnostic accuracy of early rCTP, incremental value beyond obstructive coronary artery disease (CAD; ≥50% stenosis), and compared early rCTP to late stress SPECT-MPI in patients with CAD presenting with suspicion of ACS to the emergency department.
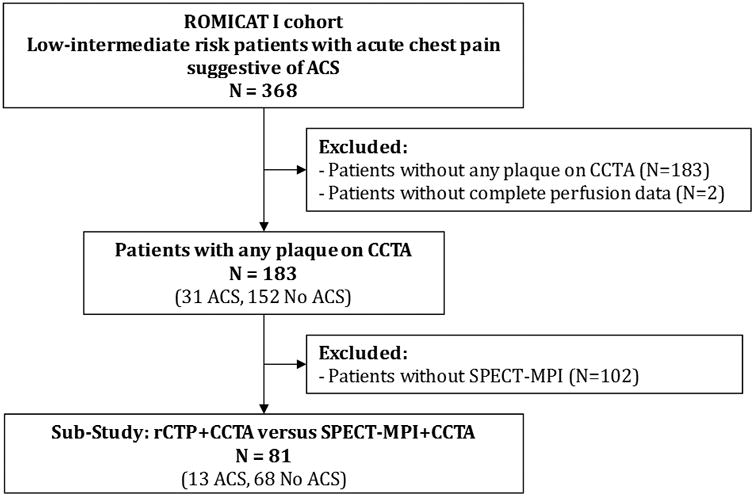
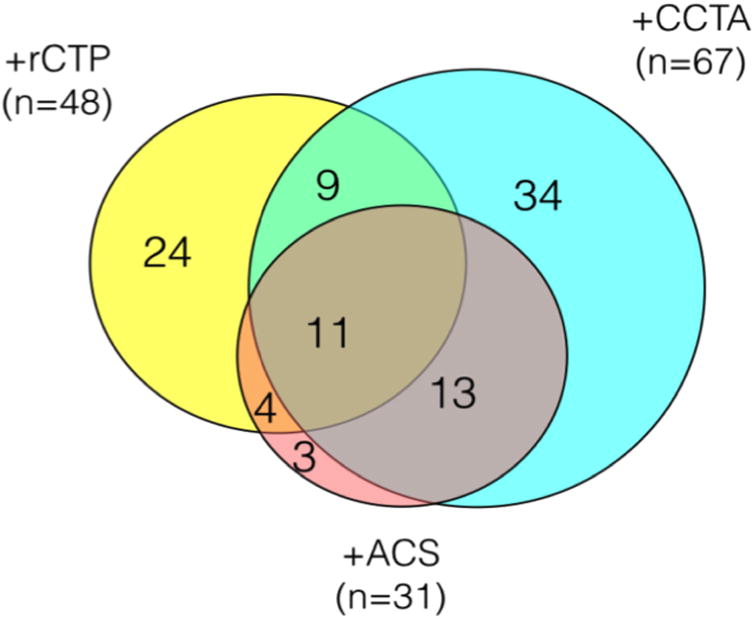
In this prespecified subanalysis of 183 patients (58.1±10.2 years; 33% women), we included patients with any CAD by coronary computed tomography angiography (CCTA) from Rule Out Myocardial Infarction Using Computer-Assisted Tomography I. rCTP was assessed semiquantitatively, blinded to CAD interpretation. Overall, 31 had ACS and 48 had abnormal rCTP. Sensitivity and specificity of rCTP for ACS were 48% (95% confidence interval [CI], 30%-67%) and 78% (95% CI, 71%-85%), respectively. rCTP predicted ACS (adjusted odds ratio, 3.40 [95% CI, 1.37-8.42]; P=0.008) independently of obstructive CAD, and sensitivity for ACS increased from 77% (95% CI, 59%-90%) for obstructive CAD to 90% (95% CI, 74%-98%) with addition of rCTP (P=0.05). In a subgroup undergoing late rest/stress SPECT-MPI (n=81), CCTA/rCTP had noninferior discriminatory value to CCTA/SPECT-MPI (area under the curve, 0.88 versus 0.90; P=0.64) using a noninferiority margin of 10%.
Early rCTP provides incremental value beyond obstructive CAD to detect ACS. CCTA/rCTP is noninferior to CCTA/SPECT-MPI to discriminate ACS and presents an attractive alternative to triage patients presenting with acute chest pain.
http://www.clinicaltrials.gov. Unique identifier: NCT00990262.
急性静息单光子发射计算机断层扫描心肌灌注成像(SPECT-MPI)对急诊科患者的急性冠状动脉综合征(ACS)具有较高的预测价值。既往研究表明,静息/负荷计算机断层扫描灌注(CTP)与SPECT-MPI之间具有良好的一致性,但静息CTP(rCTP)在急性胸痛分诊中的价值仍不明确。我们旨在确定早期rCTP的诊断准确性、在阻塞性冠状动脉疾病(CAD;狭窄≥50%)之外的增量价值,并将早期rCTP与急诊科疑似ACS的CAD患者的晚期负荷SPECT-MPI进行比较。
在对183例患者(58.1±10.2岁;33%为女性)进行的这项预先设定的亚组分析中,我们纳入了来自“使用计算机辅助断层扫描排除心肌梗死I”研究中通过冠状动脉计算机断层扫描血管造影(CCTA)诊断为任何CAD的患者。rCTP采用半定量评估,对CAD的解读结果保密。总体而言,31例患有ACS,48例rCTP异常。rCTP对ACS的敏感性和特异性分别为48%(95%置信区间[CI],30%-67%)和78%(95%CI,71%-85%)。rCTP独立于阻塞性CAD预测ACS(调整后的优势比为3.40[95%CI,1.37-8.42];P=0.008),并且添加rCTP后,ACS的敏感性从阻塞性CAD的77%(95%CI,59%-90%)提高到90%(95%CI,74%-98%)(P=0.05)。在接受晚期静息/负荷SPECT-MPI的亚组(n=81)中,使用10%的非劣效性界值,CCTA/rCTP与CCTA/SPECT-MPI的鉴别价值相当(曲线下面积分别为0.88和0.90;P=0.64)。
早期rCTP在检测ACS方面提供了阻塞性CAD之外的增量价值。CCTA/rCTP在鉴别ACS方面不劣于CCTA/SPECT-MPI,为急性胸痛患者的分诊提供了一种有吸引力的替代方法。