Ding Ann, Osorio Marcela, Teferi Maranatha, Gallo Marin Benjamin, Cruz-Sánchez Margarita, Lorenz Matthew, Michelow Ian C
Warren Alpert Medical School of Brown University, Providence, Rhode Island, USA.
Department of Pediatrics, Rhode Island Hospital, Providence, Rhode Island, USA.
Open Forum Infect Dis. 2024 Jul 19;11(8):ofae430. doi: 10.1093/ofid/ofae430. eCollection 2024 Aug.
Refugees to the United States frequently have parasitic infections. If untreated, parasites can cause severe complications. The purpose of this study was to investigate the incidence, management, and outcomes of eosinophilia as a biomarker for parasites.
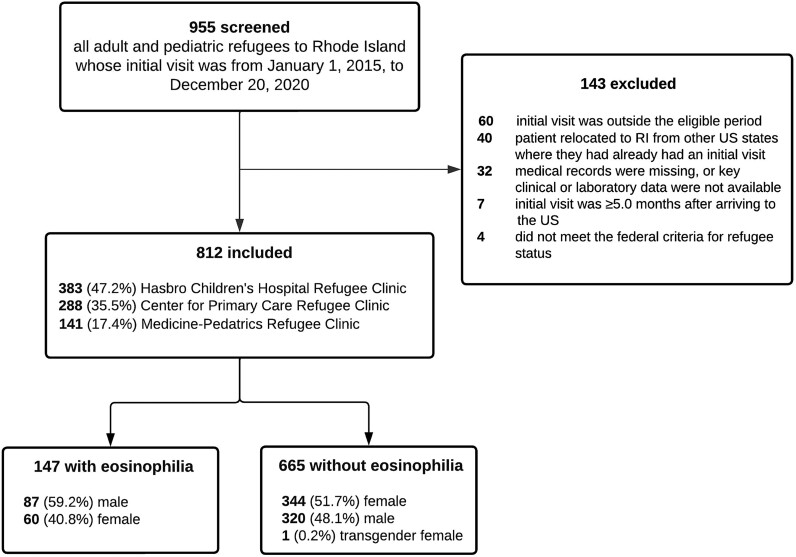
We conducted a retrospective longitudinal chart review of consecutive refugees attending 3 refugee clinics in Rhode Island that manage the health care of all pediatric and adult refugees.
Among 812 refugees who met inclusion criteria, 147 (18.1%) had eosinophilia upon arrival and almost half had ≥1 symptom. The rates and severity of eosinophilia in those with predeparture presumptive treatment records who did (112/115, 97.4%) or did not (488/498, 98.0%) receive predeparture antiparasitic treatment were similar. All refugees with eosinophilia had ≥1 parasitic test in the United States. The most common attributable parasites were and . Overall, parasites were detected in 63 (42.9%) of 147 refugees with eosinophilia by either stool testing, serology, or blood smear, but testing was inconsistent and likely underestimated true incidence. Only some of the identified parasites typically cause eosinophilia. Forty-five (30.6%) refugees with eosinophilia received antiparasitics in the United States. Of 81 (55.1%) individuals who had repeat blood tests, eosinophilia had resolved in 52 (64.2%). Five individuals (3.4%) had alternative diagnoses, including eczema, myelofibrosis, and drug allergy.
Our findings support Centers for Disease Control and Prevention recommendations to screen for eosinophilia in newly arrived refugees. Follow-up after 3-6 months is critical to confirm resolution of residual eosinophilia, which frequently occurs after effective predeparture treatment or if eosinophilia persists, to diagnose active parasitic infections.
前往美国的难民经常患有寄生虫感染。如果不进行治疗,寄生虫会导致严重并发症。本研究的目的是调查嗜酸性粒细胞增多作为寄生虫生物标志物的发生率、管理及结果。
我们对在罗德岛3家为难所有儿科和成人难民提供医疗保健服务的难民诊所就诊的连续难民进行了回顾性纵向病历审查。
在812名符合纳入标准的难民中,147人(18.1%)抵达时患有嗜酸性粒细胞增多症,且近一半有≥1种症状。有出发前推定治疗记录且接受(112/115,97.4%)或未接受(488/498,98.0%)出发前抗寄生虫治疗者的嗜酸性粒细胞增多症发生率及严重程度相似。所有嗜酸性粒细胞增多的难民在美国都进行了≥1次寄生虫检测。最常见的致病寄生虫是 和 。总体而言,通过粪便检测、血清学或血涂片,在147名嗜酸性粒细胞增多的难民中有63人(42.9%)检测到寄生虫,但检测不一致,可能低估了实际发生率。只有部分已识别的寄生虫通常会导致嗜酸性粒细胞增多。45名(30.6%)嗜酸性粒细胞增多的难民在美国接受了抗寄生虫治疗。在81名(55.1%)进行了重复血液检测的个体中,52人(64.2%)的嗜酸性粒细胞增多症已缓解。5名个体(3.4%)有其他诊断,包括湿疹、骨髓纤维化和药物过敏。
我们的研究结果支持疾病控制与预防中心对新抵达难民进行嗜酸性粒细胞增多症筛查的建议。3至六个月后的随访对于确认残留嗜酸性粒细胞增多症是否缓解至关重要,残留嗜酸性粒细胞增多症常在有效的出发前治疗后出现,或者如果嗜酸性粒细胞增多症持续存在,则对于诊断活动性寄生虫感染至关重要。