Department of Cardiology, The Heart Center, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark.
Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark.
Intensive Care Med. 2024 Sep;50(9):1484-1495. doi: 10.1007/s00134-024-07574-6. Epub 2024 Aug 20.
Out-of-hospital cardiac arrest (OHCA) survivors face significant risks of complications and death from hypoxic-ischemic brain injury leading to withdrawal of life-sustaining treatment (WLST). Accurate multimodal neuroprognostication, including automated pupillometry, is essential to avoid inappropriate WLST. However, inconsistent study results hinder standardized threshold recommendations. We aimed to validate proposed pupillometry thresholds with no false predictions of unfavorable outcomes in comatose OHCA survivors.
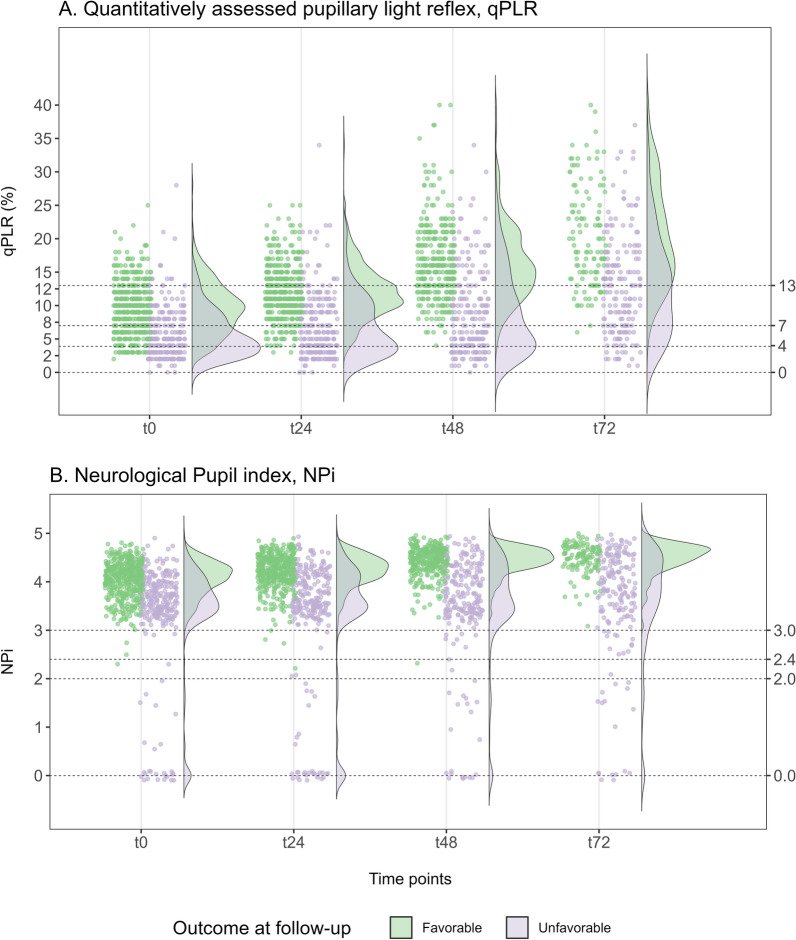
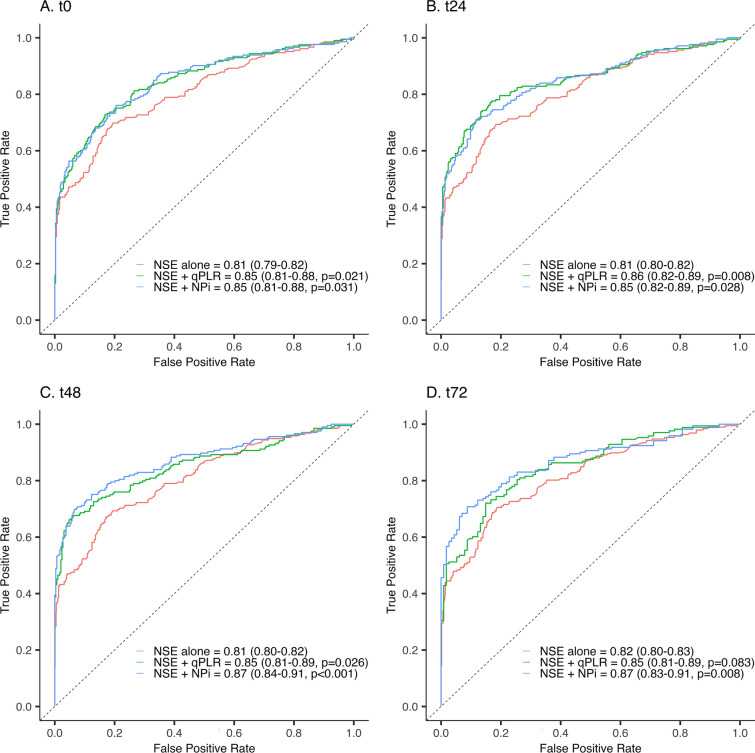
In the multi-center BOX-trial, quantitative measurements of automated pupillometry (quantitatively assessed pupillary light reflex [qPLR] and Neurological Pupil index [NPi]) were obtained at admission (0 h) and after 24, 48, and 72 h in comatose patients resuscitated from OHCA. We aimed to validate qPLR < 4% and NPi ≤ 2, predicting unfavorable neurological conditions defined as Cerebral Performance Category 3-5 at follow-up. Combined with 48-h neuron-specific enolase (NSE) > 60 μg/L, pupillometry was evaluated for multimodal neuroprognostication in comatose patients with Glasgow Motor Score (M) ≤ 3 at ≥ 72 h.
From March 2017 to December 2021, we consecutively enrolled 710 OHCA survivors (mean age: 63 ± 14 years; 82% males), and 266 (37%) patients had unfavorable neurological outcomes. An NPi ≤ 2 predicted outcome with 0% false-positive rate (FPR) at all time points (0-72 h), and qPLR < 4% at 24-72 h. In patients with M ≤ 3 at ≥ 72 h, pupillometry thresholds significantly increased the sensitivity of NSE, from 42% (35-51%) to 55% (47-63%) for qPLR and 50% (42-58%) for NPi, maintaining 0% (0-0%) FPR.
Quantitative pupillometry thresholds predict unfavorable neurological outcomes in comatose OHCA survivors and increase the sensitivity of NSE in a multimodal approach at ≥ 72 h.
院外心脏骤停(OHCA)幸存者由于缺氧缺血性脑损伤面临着严重的并发症和死亡风险,这可能导致停止维持生命的治疗(WLST)。准确的多模式神经预后评估,包括自动瞳孔测量,对于避免不适当的 WLST 至关重要。然而,不一致的研究结果阻碍了标准化阈值建议。我们旨在验证提出的瞳孔测量阈值,即在昏迷的 OHCA 幸存者中没有预测不良结局的假阳性。
在多中心 BOX 试验中,在 OHCA 复苏后昏迷的患者入院时(0 小时)和 24、48 和 72 小时时获得自动瞳孔测量(定量评估瞳孔光反射[qPLR]和神经瞳孔指数[NPi])的定量测量。我们旨在验证 qPLR < 4%和 NPi ≤ 2 可预测不良神经状况,定义为随访时的脑功能分类 3-5。结合 48 小时神经元特异性烯醇化酶(NSE)> 60 μg/L,在格拉斯哥运动评分(M)≤ 3 且≥ 72 小时的昏迷患者中,评估瞳孔测量的多模式神经预后。
从 2017 年 3 月至 2021 年 12 月,我们连续纳入 710 例 OHCA 幸存者(平均年龄:63 ± 14 岁;82%为男性),266 例(37%)患者存在不良神经结局。NPi ≤ 2 在所有时间点(0-72 小时)均具有 0%的假阳性率(FPR)预测结局,而 qPLR < 4%在 24-72 小时。在 M≤ 3 且≥ 72 小时的患者中,瞳孔测量阈值显著提高了 NSE 的敏感性,从 qPLR 的 42%(35-51%)增加到 55%(47-63%),NPi 增加到 50%(42-58%),同时保持 0%(0-0%)的 FPR。
定量瞳孔测量阈值可预测昏迷的 OHCA 幸存者的不良神经结局,并在≥72 小时的多模态方法中提高 NSE 的敏感性。