Hsu Wei-Hsiang, Wang San-Yuan, Chao Yen-Ming, Chang Ke-Vin, Han Der-Sheng, Lin Yun-Lian
Department of Chinese Pharmaceutical Sciences and Chinese Medicine Resources, China Medical University, Taichung, Taiwan.
Institute of Biopharmaceutical Sciences, National Yang-Ming-Chiao-Tung University, Taipei, Taiwan.
J Cachexia Sarcopenia Muscle. 2024 Oct;15(5):2175-2186. doi: 10.1002/jcsm.13567. Epub 2024 Aug 21.
The pathophysiology of sarcopenia is complex and multifactorial and has not been fully elucidated. The impact of resistance training and nutritional support (RTNS) on metabolomics and lipodomics in older adults with sarcopenia remains uncertain. This study aimed to explore potential biomarkers of sarcopenia and clinical indicators of RTNS in older sarcopenic adults.
Older individuals diagnosed with sarcopenia through routine health checkups at a community hospital were recruited for a 12-week randomized controlled trial focusing on RTNS. Plasma metabolomic and lipidomic profiles of 45 patients with sarcopenia and 47 matched controls were analysed using H-nuclear magnetic resonance (H-NMR) and liquid chromatography-mass spectrometer (LC-MS).
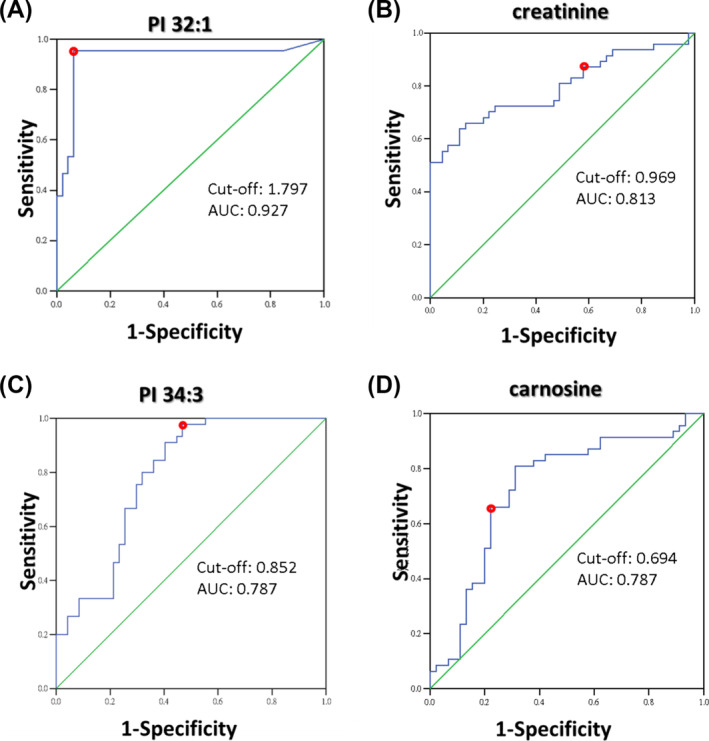
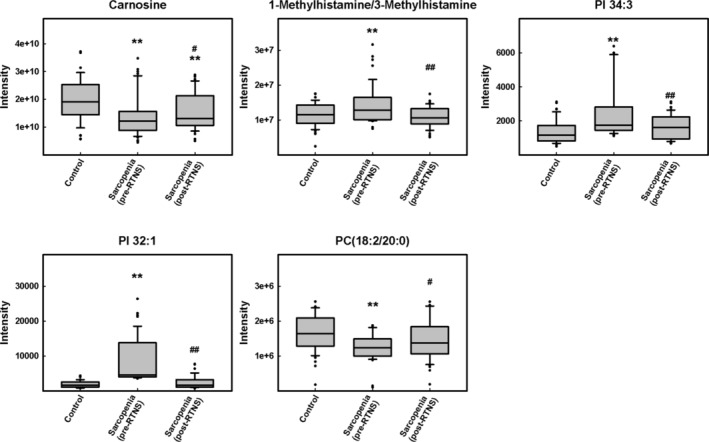
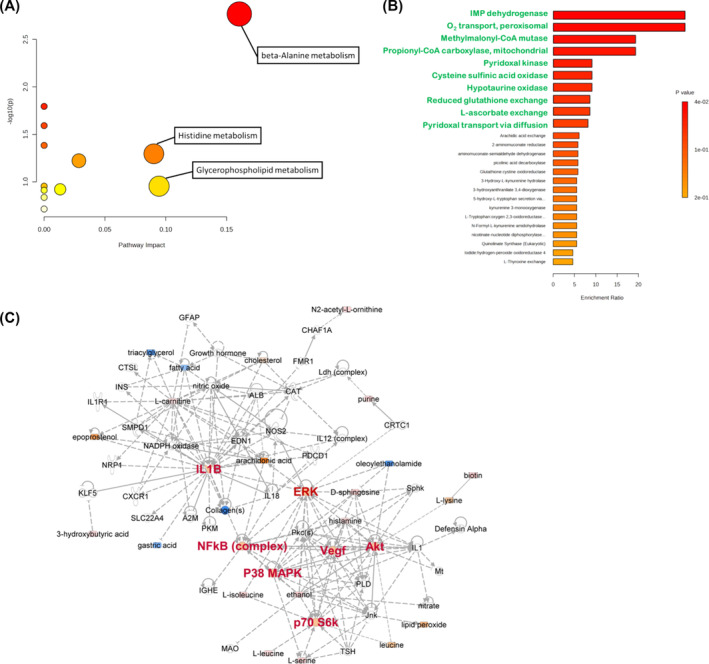
At baseline, the patient and control groups had similar age, sex, and height distribution. The patient group had significantly lower weight, BMI, grip strength, gait speed, skeletal muscle index, lean mass of both the upper and lower limbs, and lower limb bone mass. There was a significant difference in 12 metabolites between the control and patient groups. They are isoleucine (patient/control fold change [FC] = 0.86 ± 0.04, P = 0.0005), carnitine (FC = 1.05 ± 0.01, P = 0.0110), 1-methylhistamine/3-methylhistamine (FC = 1.24 ± 0.14, P = 0.0039), creatinine (FC = 0.71 ± 0.04, P < 0.0001), carnosine (FC = 0.71 ± 0.04, P = 0.0007), ureidopropionic acid (FC = 0.61 ± 0.10, P = 0.0107), uric acid (FC = 0.88 ± 0.03, P = 0.0083), PC (18:2/20:0) (FC = 0.69 ± 0.03, P = 0.0010), PC (20:2/18:0) (FC = 0.70 ± 0.06, P = 0.0014), PC (18:1/20:1) (FC = 0.74 ± 0.05, P = 0.0015), PI 32:1 (FC = 4.72 ± 0.17, P = 0.0006), and PI 34:3 (FC = 1.88 ± 0.13, P = 0.0003). Among them, carnitine, 1-methylhistamine/3-methylhistamine, creatinine, ureidopropionic acid, uric acid, PI 32:1, and PI 34:3 were first identified. Notably, PI 32:1 had highest diagnostic accuracy (0.938) for sarcopenia. 1-Methylhistamine/3-methylhistamine, carnosine, PC (18:2/20:0), PI 32:1, and PI 34:3 levels were not different from the control group after RTNS. These metabolites are involved in amino acid metabolism, lipid metabolism, and the PI3K-AKT/mTOR signalling pathway through the ingenuity pathway analysis.
These findings provide information on metabolic changes, lipid perturbations, and the role of RTNS in patients with sarcopenia. They reveal new insights into its pathological mechanisms and potential therapies.
肌肉减少症的病理生理学复杂且多因素,尚未完全阐明。抗阻训练和营养支持(RTNS)对老年肌肉减少症患者代谢组学和脂质组学的影响仍不确定。本研究旨在探索老年肌肉减少症患者肌肉减少症的潜在生物标志物和RTNS的临床指标。
通过社区医院常规健康检查诊断为肌肉减少症的老年人被招募参加一项为期12周的聚焦于RTNS的随机对照试验。使用氢核磁共振(H-NMR)和液相色谱-质谱仪(LC-MS)分析了45例肌肉减少症患者和47例匹配对照的血浆代谢组学和脂质组学谱。
在基线时,患者组和对照组在年龄、性别和身高分布方面相似。患者组的体重、体重指数、握力、步速、骨骼肌指数、上下肢瘦体重和下肢骨量显著更低。对照组和患者组之间有12种代谢物存在显著差异。它们是异亮氨酸(患者/对照倍数变化[FC]=0.86±0.04,P=0.0005)、肉碱(FC=1.05±0.01,P=0.0110)、1-甲基组胺/3-甲基组胺(FC=1.24±0.14,P=0.0039)、肌酐(FC=0.71±0.04,P<0.0001)、肌肽(FC=0.71±0.04,P=0.0007)、脲基丙酸(FC=0.61±0.10,P=0.0107)、尿酸(FC=0.88±0.03,P=0.0083)、PC(18: