Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom.
Peninsula Medical School, University of Plymouth, Plymouth, United Kingdom.
J Med Internet Res. 2024 Aug 26;26:e56042. doi: 10.2196/56042.
No single multimorbidity measure is validated for use in NHS (National Health Service) England's General Practice Extraction Service Data for Pandemic Planning and Research (GDPPR), the nationwide primary care data set created for COVID-19 pandemic research. The Cambridge Multimorbidity Score (CMMS) is a validated tool for predicting mortality risk, with 37 conditions defined by Read Codes. The GDPPR uses the more internationally used Systematized Nomenclature of Medicine clinical terms (SNOMED CT). We previously developed a modified version of the CMMS using SNOMED CT, but the number of terms for the GDPPR data set is limited making it impossible to use this version.
We aimed to develop and validate a modified version of CMMS using the clinical terms available for the GDPPR.
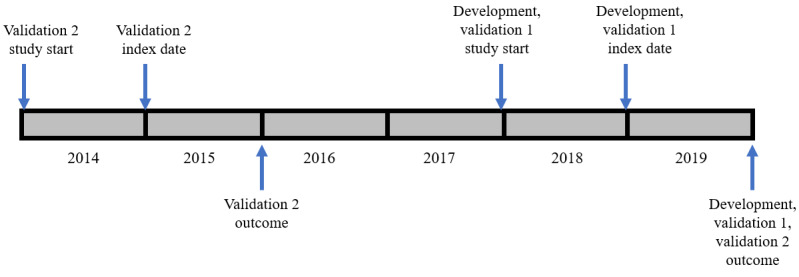
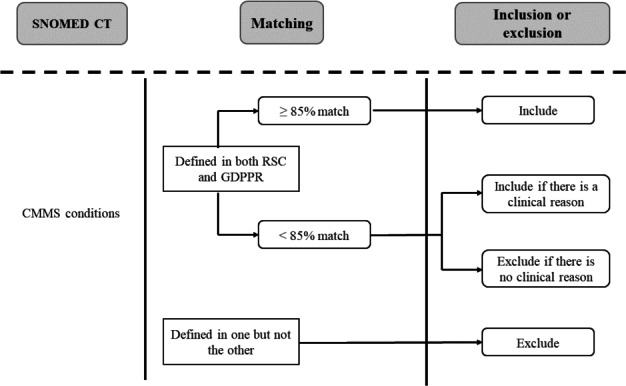
We used pseudonymized data from the Oxford-Royal College of General Practitioners Research and Surveillance Centre (RSC), which has an extensive SNOMED CT list. From the 37 conditions in the original CMMS model, we selected conditions either with (1) high prevalence ratio (≥85%), calculated as the prevalence in the RSC data set but using the GDPPR set of SNOMED CT codes, divided by the prevalence included in the RSC SNOMED CT codes or (2) conditions with lower prevalence ratios but with high predictive value. The resulting set of conditions was included in Cox proportional hazard models to determine the 1-year mortality risk in a development data set (n=500,000) and construct a new CMMS model, following the methods for the original CMMS study, with variable reduction and parsimony, achieved by backward elimination and the Akaike information stopping criterion. Model validation involved obtaining 1-year mortality estimates for a synchronous data set (n=250,000) and 1-year and 5-year mortality estimates for an asynchronous data set (n=250,000). We compared the performance with that of the original CMMS and the modified CMMS that we previously developed using RSC data.
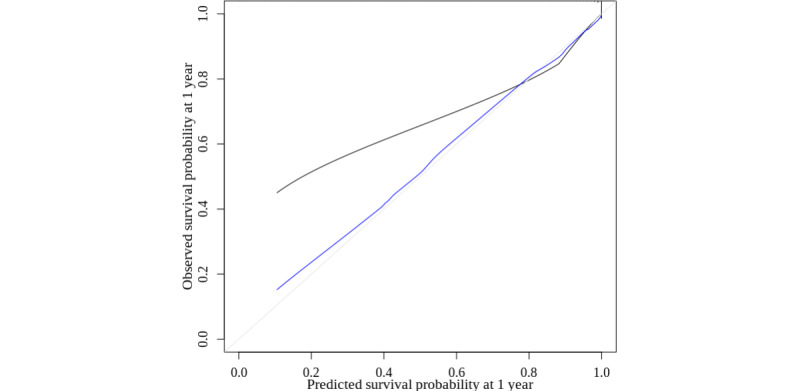
The initial model contained 22 conditions and our final model included 17 conditions. The conditions overlapped with those of the modified CMMS using the more extensive SNOMED CT list. For 1-year mortality, discrimination was high in both the derivation and validation data sets (Harrell C=0.92) and 5-year mortality was slightly lower (Harrell C=0.90). Calibration was reasonable following an adjustment for overfitting. The performance was similar to that of both the original and previous modified CMMS models.
The new modified version of the CMMS can be used on the GDPPR, a nationwide primary care data set of 54 million people, to enable adjustment for multimorbidity in predicting mortality in people in real-world vaccine effectiveness, pandemic planning, and other research studies. It requires 17 variables to produce a comparable performance with our previous modification of CMMS to enable it to be used in routine data using SNOMED CT.
没有单一的多病种衡量标准经过验证可用于 NHS(国家医疗服务体系)英格兰的全科医生提取服务数据用于大流行规划和研究(GDPPR),这是为 COVID-19 大流行研究创建的全国性初级保健数据集。剑桥多病种评分(CMMS)是一种经过验证的预测死亡率风险的工具,其中 37 种疾病由 Read 代码定义。GDPPR 使用更国际化的医学系统术语命名法(SNOMED CT)。我们之前使用 SNOMED CT 开发了 CMMS 的修改版本,但 GDPPR 数据集的术语数量有限,无法使用此版本。
我们旨在使用 GDPPR 可用的临床术语开发和验证 CMMS 的修改版本。
我们使用来自牛津皇家全科医生研究和监测中心(RSC)的假名化数据,该中心拥有广泛的 SNOMED CT 清单。在原始 CMMS 模型中的 37 种疾病中,我们选择了以下两种疾病:(1)高流行率比(≥85%),按照 RSC 数据集中的流行率计算,但使用 GDPPR 的 SNOMED CT 代码集除以 RSC SNOMED CT 代码中包含的流行率;或(2)流行率比较低但预测值较高的疾病。将由此产生的疾病集包含在 Cox 比例风险模型中,以确定开发数据集(n=500,000)中的 1 年死亡率风险,并根据原始 CMMS 研究的方法构建新的 CMMS 模型,通过向后消除和 Akaike 信息停止准则实现变量减少和简约。模型验证涉及为同步数据集(n=250,000)获取 1 年死亡率估计值,并为异步数据集(n=250,000)获取 1 年和 5 年死亡率估计值。我们将性能与原始 CMMS 和我们之前使用 RSC 数据开发的修改后的 CMMS 进行了比较。
初始模型包含 22 种疾病,我们的最终模型包含 17 种疾病。这些疾病与使用更广泛的 SNOMED CT 清单的修改后的 CMMS 中的疾病重叠。对于 1 年死亡率,推导和验证数据集中的区分度都很高(Harrell C=0.92),5 年死亡率略低(Harrell C=0.90)。经过过度拟合调整后,校准是合理的。该性能与原始和以前的修改后的 CMMS 模型相似。
新的 CMMS 修改版本可用于 GDPPR,这是一个拥有 5400 万人口的全国性初级保健数据集,可用于调整多病种在预测现实世界疫苗有效性、大流行规划和其他研究研究中人群死亡率方面的影响。它需要 17 个变量才能产生与我们之前对 CMMS 的修改版本相当的性能,从而能够在常规数据中使用 SNOMED CT 进行使用。