Department of Psychology, University of Michigan, Ann Arbor.
Yale University, New Haven, Connecticut.
JAMA Netw Open. 2024 Aug 1;7(8):e2430711. doi: 10.1001/jamanetworkopen.2024.30711.
Adverse childhood experiences are pervasive and heterogeneous, with potential lifelong consequences for psychiatric morbidity and brain health. Existing research does not capture the complex interplay of multiple adversities, resulting in a lack of precision in understanding their associations with neural function and mental health.
To identify distinct childhood adversity profiles and examine their associations with adolescent mental health and brain connectivity.
DESIGN, SETTING, AND PARTICIPANTS: This population-based birth cohort used data for children who were born in 20 large US cities between 1998 and 2000 and participated in the Future Families and Child Well-Being Study. Families were interviewed when children were born and at ages 1, 3, 5, 9, and 15 years. At age 15 years, neuroimaging data were collected from a subset of these youths. Data were collected from February 1998 to April 2017. Analyses were conducted from March to December 2023.
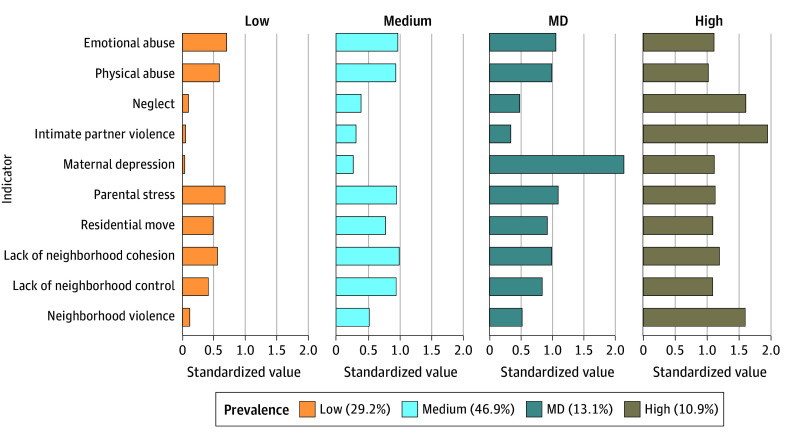
Latent profiles of childhood adversity, defined by family and neighborhood risks across ages 0 to 9 years.
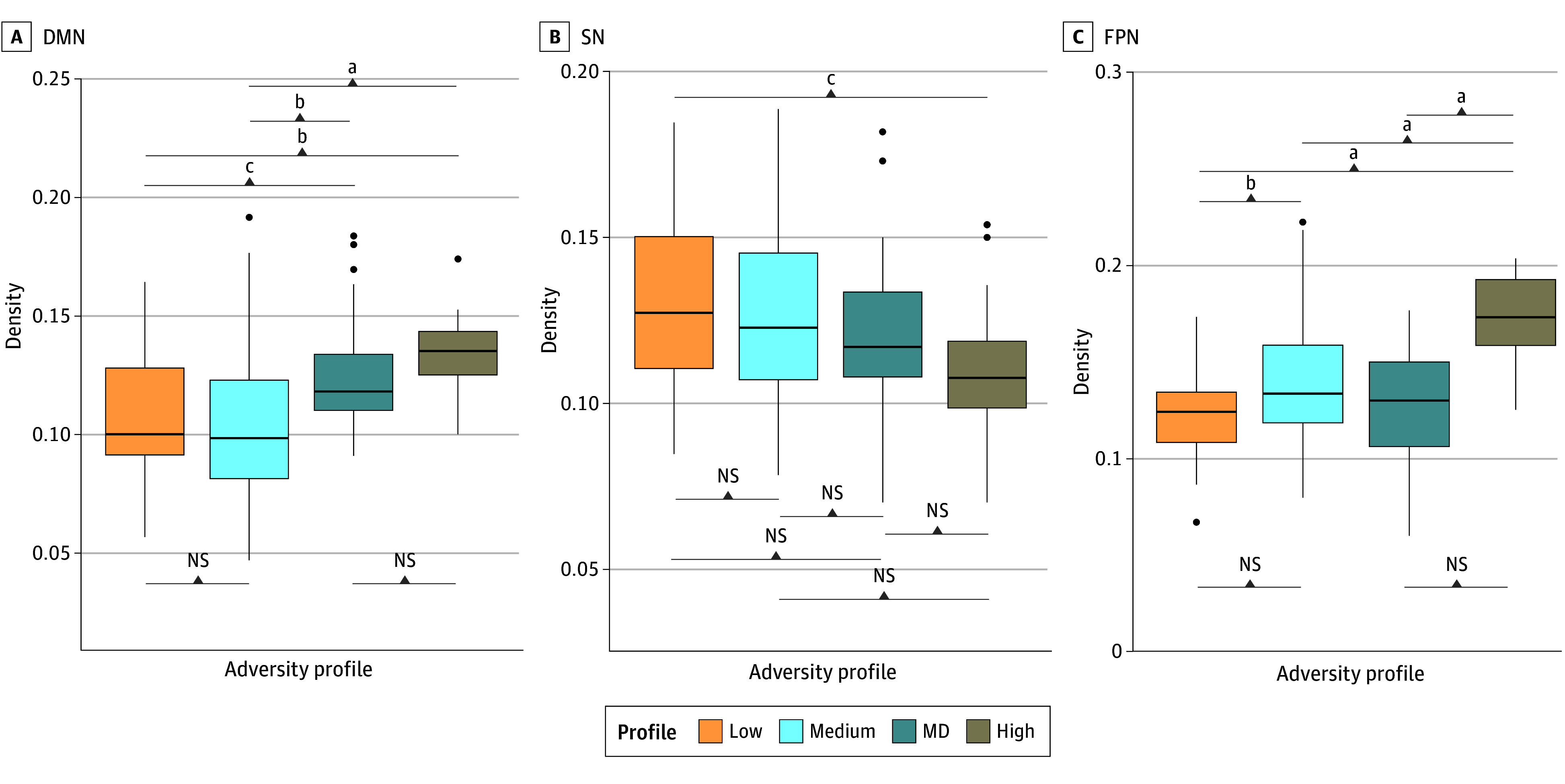
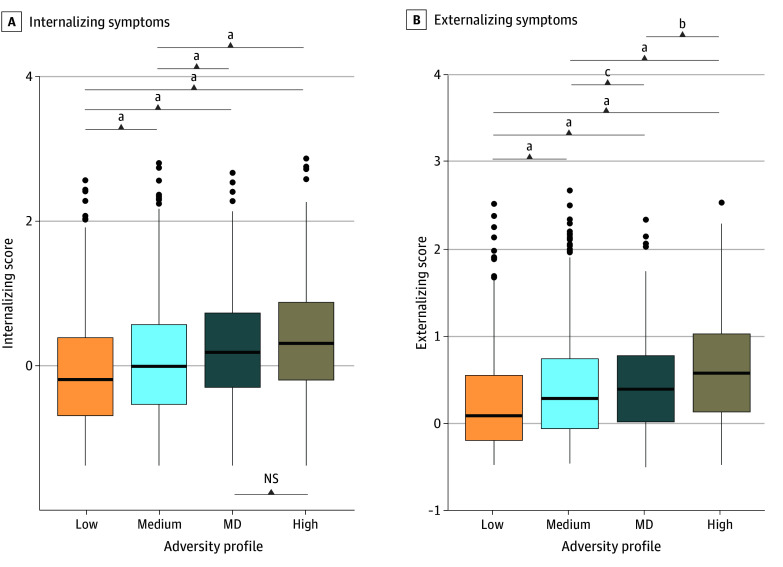
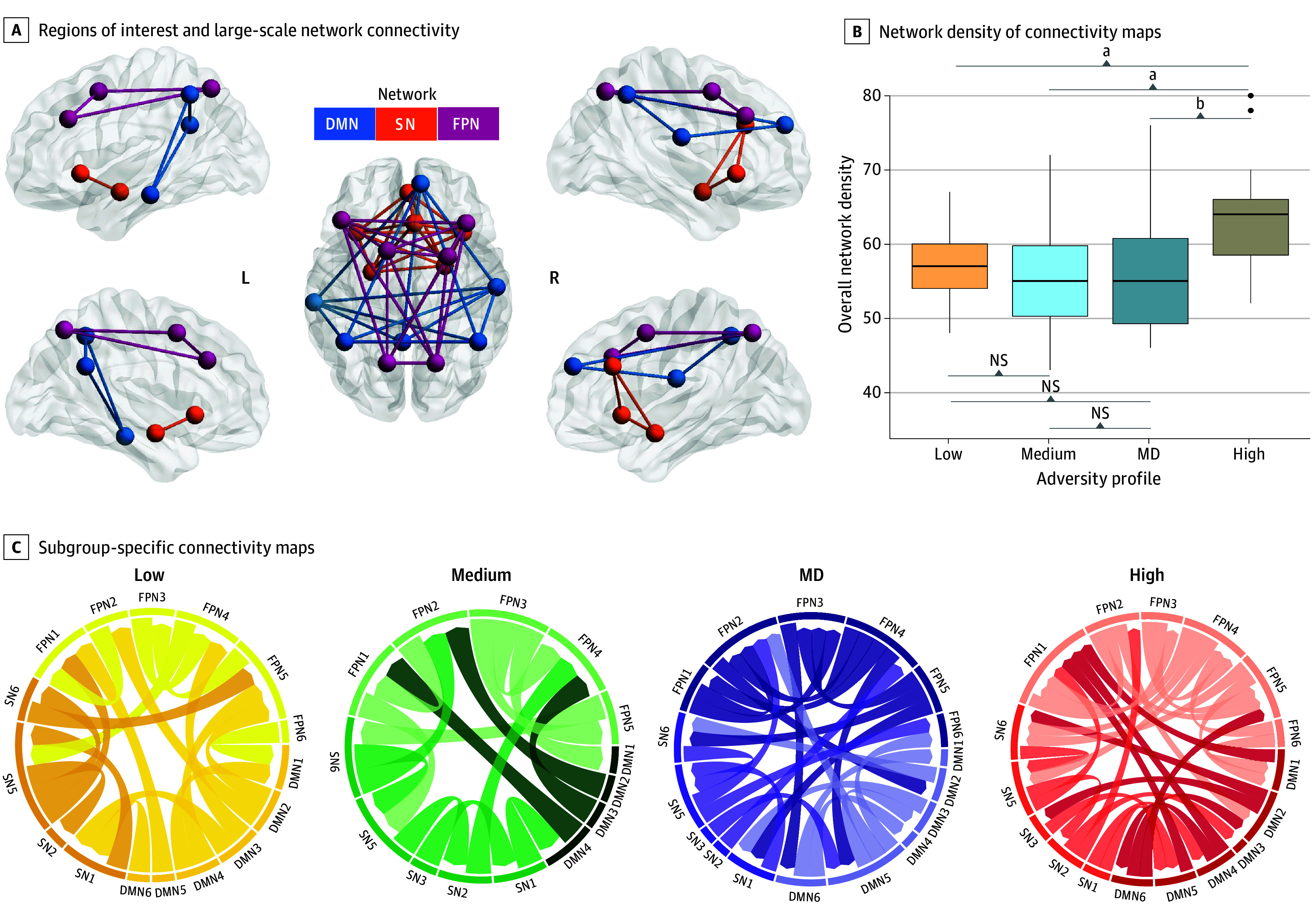
Internalizing and externalizing symptoms at age 15 years using parent- and youth-reported measures. Profile-specific functional magnetic resonance imaging connectivity across the default mode network (DMN), salience network (SN), and frontoparietal network (FPN).
Data from 4210 individuals (2211 [52.5%] male; 1959 [46.5%] Black, 1169 [27.7%] Hispanic, and 786 [18.7%] White) revealed 4 childhood adversity profiles: low-adversity (1230 individuals [29.2%]), medium-adversity (1973 [46.9%]), high-adversity (457 [10.9%]), and high maternal depression (MD; 550 [13.1%]). High-adversity, followed by MD, profiles had the highest symptoms. Notably, internalizing symptoms did not differ between these 2 profiles (mean difference, 0.11; 95% CI, -0.03 to 0.26), despite the MD profile showing adversity levels most similar to the medium-adversity profile. In the neuroimaging subsample of 167 individuals (91 [54.5%] female; 128 [76.6%] Black, 11 [6.6%] Hispanic, and 20 [12.0%] White; mean [SD] age, 15.9 [0.5] years), high-adversity and MD profiles had the highest DMN density relative to other profiles (F(3,163) = 11.14; P < .001). The high-adversity profile had lower SN density relative to the low-adversity profile (mean difference, -0.02; 95% CI, -0.04 to -0.003) and the highest FPN density among all profiles (F(3,163) = 18.96; P < .001). These differences were specific to brain connectivity during an emotion task, but not at rest.
In this cohort study, children who experienced multiple adversities, or only elevated MD, had worse mental health and different neural connectivity in adolescence. Interventions targeting multiple risk factors, with a focus on maternal mental health, could produce the greatest benefits.
童年逆境普遍存在且具有异质性,可能对精神疾病发病率和大脑健康产生终身影响。现有研究无法捕捉到多种逆境的复杂相互作用,导致对其与神经功能和心理健康之间关系的理解缺乏准确性。
确定不同的童年逆境特征,并研究其与青少年心理健康和大脑连接的关系。
设计、地点和参与者:这项基于人群的出生队列研究使用了 1998 年至 2000 年期间在美国 20 个大城市出生的儿童的数据,并参加了未来家庭和儿童福祉研究。当孩子出生时以及在 1、3、5、9 和 15 岁时对家庭进行了访谈。在这些年轻人中,有一部分人在 15 岁时进行了神经影像学数据采集。数据收集时间为 1998 年 2 月至 2017 年 4 月。分析时间为 2023 年 3 月至 12 月。
0 至 9 岁时家庭和邻里风险的儿童逆境特征。
使用父母和青少年报告的措施,在 15 岁时评估内在和外在症状。使用默认模式网络 (DMN)、突显网络 (SN) 和额顶网络 (FPN) 的特定于特征的功能磁共振成像连接。
来自 4210 名个体(2211 [52.5%] 为男性;1959 [46.5%] 为黑人,1169 [27.7%] 为西班牙裔,786 [18.7%] 为白人)的数据显示了 4 种童年逆境特征:低逆境(1230 人 [29.2%])、中逆境(1973 人 [46.9%])、高逆境(457 人 [10.9%])和高母抑郁(MD;550 人 [13.1%])。高逆境和 MD 特征的个体表现出最高的症状。值得注意的是,这两种特征之间的内在症状并没有差异(平均差异,0.11;95%CI,-0.03 至 0.26),尽管 MD 特征表现出的逆境水平与中逆境特征最为相似。在 167 名神经影像学样本个体(91 [54.5%] 为女性;128 [76.6%] 为黑人,11 [6.6%] 为西班牙裔,20 [12.0%] 为白人;平均[SD]年龄,15.9 [0.5] 岁)中,高逆境和 MD 特征与其他特征相比,DMN 密度最高(F(3,163)=11.14;P<.001)。高逆境特征的 SN 密度低于低逆境特征(平均差异,-0.02;95%CI,-0.04 至-0.003),且在所有特征中具有最高的 FPN 密度(F(3,163)=18.96;P<.001)。这些差异在情绪任务期间的大脑连接中是特异性的,但在休息时不是。
在这项队列研究中,经历多种逆境或仅经历 MD 升高的儿童在青少年时期的心理健康和大脑连接较差。针对多种风险因素的干预措施,重点关注产妇心理健康,可能会产生最大的益处。