Pesaresi Alessandro, La Cava Pietro, Bonada Marta, Zeppa Pietro, Melcarne Antonio, Cofano Fabio, Fiaschi Pietro, Garbossa Diego, Bianconi Andrea
Neurosurgery Unit, Department of Neuroscience, University of Turin, Via Cherasco 15, 10126 Turin, Italy.
Department of Neurosurgery, Fondazione IRCCS Istituto Neurologico Carlo Besta, Via Celoria 11, 20133 Milan, Italy.
Cancers (Basel). 2024 Aug 6;16(16):2771. doi: 10.3390/cancers16162771.
Fluorescence-guided resection (FGR) of glioblastomas has been previously explored with the use of 5-amivelulinic acid (5-ALA) and sodium fluoresceine (SF), allowing us to maximize the extent of resection (EoR). In this study, we highlight the most relevant concerns regarding this technique and present the methods and results from the experience of our center.
A case series of 100 patients operated on in AOU Città della Salute e della Scienza in Turin with a histological diagnosis of glioblastoma (grade IV, according to WHO 2021) was retrospectively analyzed. Both 5-ALA and SF were administered and intraoperatively assessed with an optical microscope.
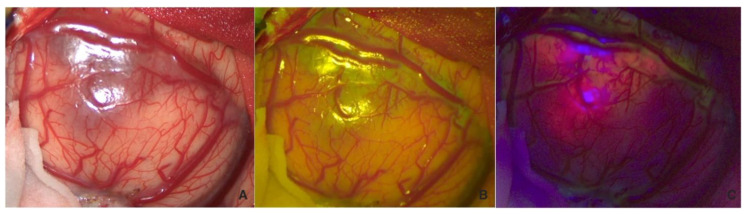
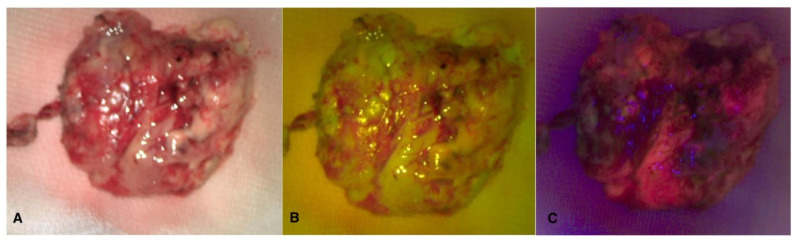
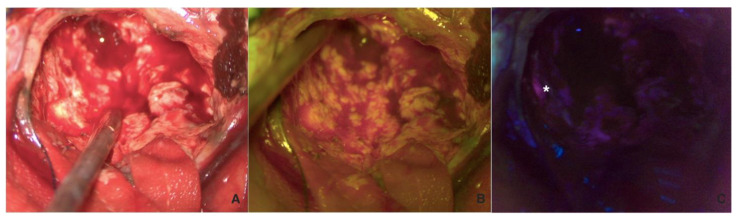
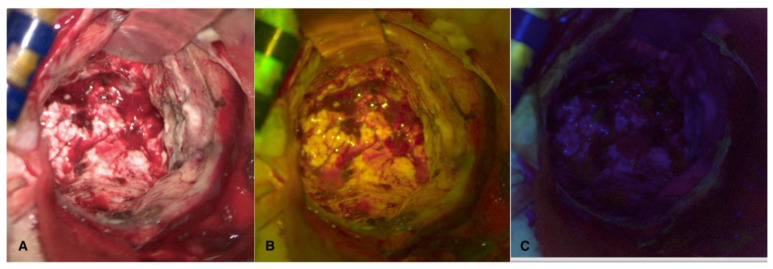
5-ALA is the only approved drug for FGR in glioblastoma, reporting an increased EoR. Nevertheless, SF can be positively used in addition to 5-ALA to reduce the risk of false positives without increasing the rate of adverse effects. In our experience, SF was used to guide the initial phase of resection while 5-ALA was used to visualize tumor spots within the surgical cavity. In 96% of cases, gross total resection was achieved, with supra-maximal resection in 11% of cases.
Combined FGR using 5-ALA and SF seems to be a promising method of increasing the extent of resection and to improving the prognosis in glioblastoma patients.
先前已使用5-氨基乙酰丙酸(5-ALA)和荧光素钠(SF)对胶质母细胞瘤进行荧光引导切除术(FGR),使我们能够最大限度地扩大切除范围(EoR)。在本研究中,我们强调了关于该技术的最相关问题,并介绍了我们中心的经验、方法和结果。
回顾性分析了在都灵的AOU Città della Salute e della Scienza接受手术的100例组织学诊断为胶质母细胞瘤(根据WHO 2021标准为IV级)的患者病例系列。同时给予5-ALA和SF,并使用光学显微镜进行术中评估。
5-ALA是胶质母细胞瘤FGR唯一获批的药物,报告显示其可提高EoR。然而,除5-ALA外,SF也可有效使用,以降低假阳性风险,且不增加不良反应发生率。根据我们的经验,SF用于引导切除的初始阶段,而5-ALA用于可视化手术腔内的肿瘤病灶。在96%的病例中实现了大体全切除,11%的病例实现了超最大切除。
联合使用5-ALA和SF的FGR似乎是一种有前景的方法,可增加胶质母细胞瘤患者的切除范围并改善预后。