Department of Urology, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, Zhejiang, China.
BMC Urol. 2024 Aug 29;24(1):185. doi: 10.1186/s12894-024-01563-z.
For localized prostate cancer, a comprehensive treatment approach centered around radical prostatectomy (RP) is often their optimal choice. Successful RP can typically reduce prostate-specific antigen (PSA) levels to below 0.1 ng/mL within 6 to 8 weeks postoperatively. However, in clinical practice, 5 to 24% of patients may have a PSA ≥ 0.1 ng/mL at 6 to 8 weeks after surgery, a phenomenon known as PSA persistence. Many studies based on data from Europe and United States have shown an association between PSA persistence and poor postoperative outcomes, further analyzing the risk factors for PSA persistence. However, relevant research based on data from China remains scarce.
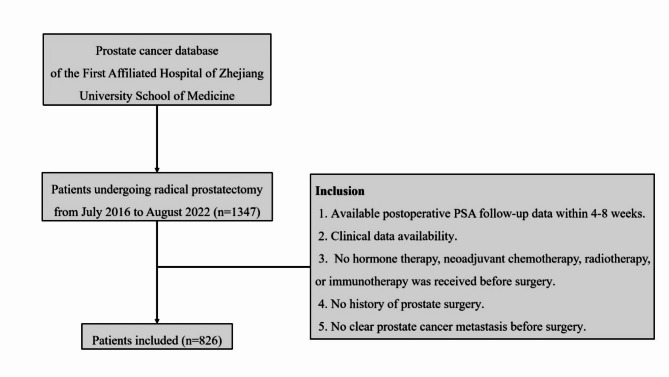
Retrospective study of 1,347 prostate cancer patients who underwent RP at the First Affiliated Hospital of Zhejiang University School of Medicine from July 15, 2016, to August 31, 2022. Based on inclusion criteria, univariate and multivariate logistic regression analyses were conducted to explore the independent risk factors for persistent PSA.
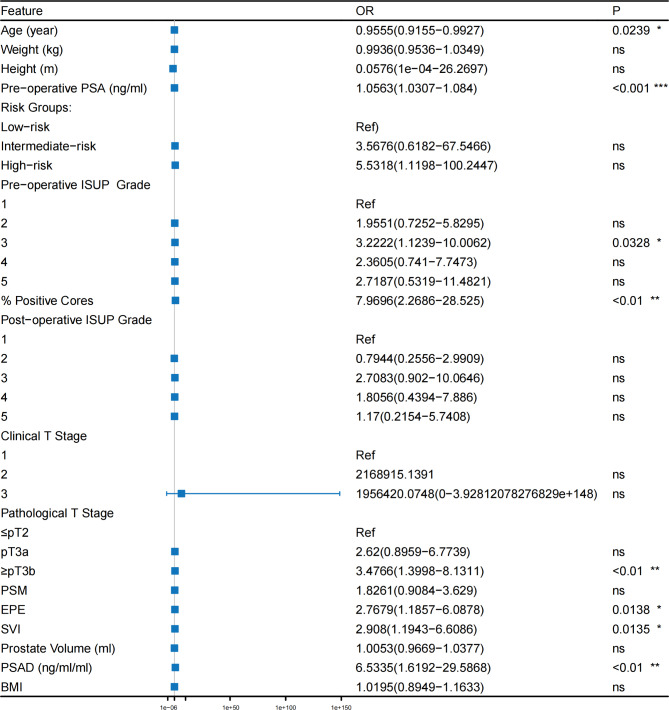
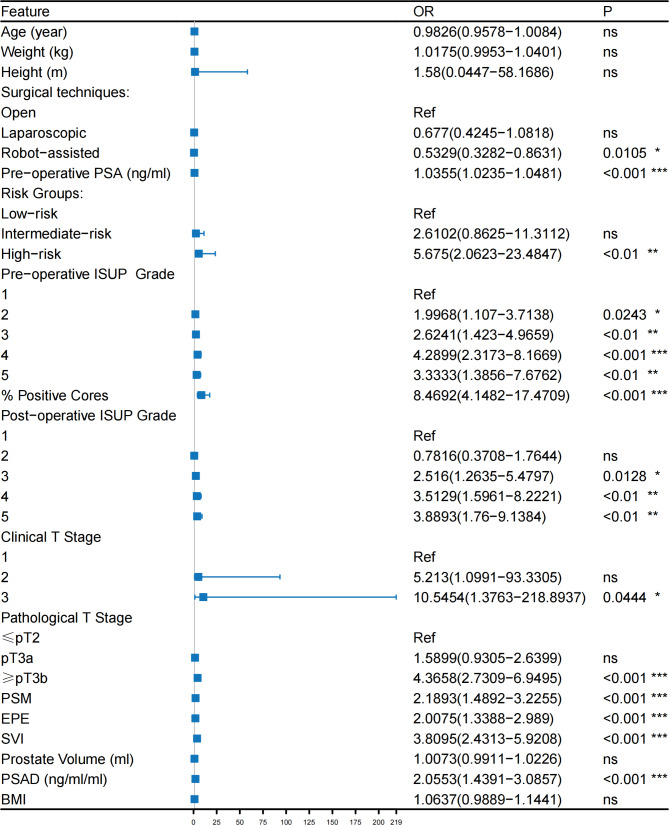
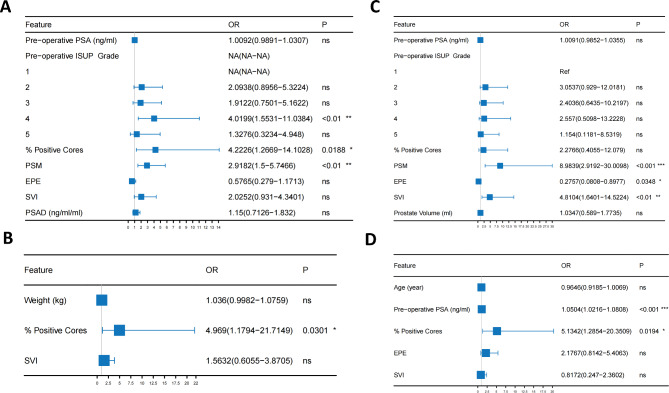
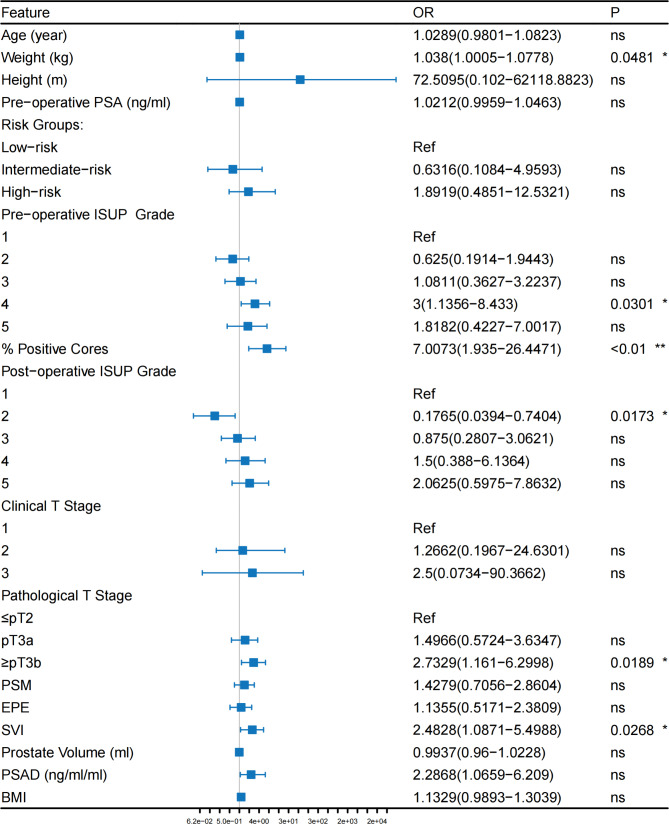
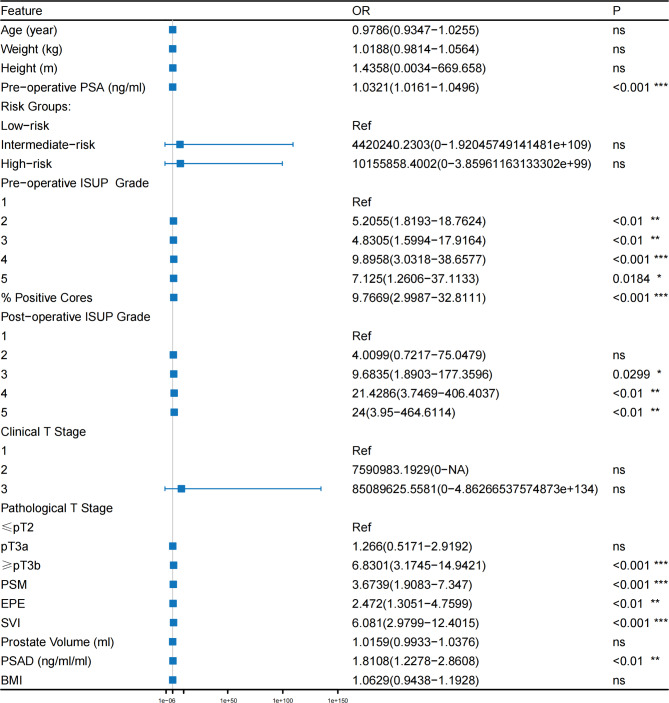
Among the 826 prostate cancer patients after RP, 124 patients experienced persistent PSA. In univariate logistic regression analysis, robot-assisted laparoscopic radical prostatectomy (RARP), preoperative PSA, high-risk group, preoperative International Society of Urological Pathology (ISUP) grades 2-5, postoperative ISUP grades 3-5, percentage of positive cores, cT3, ≥pT3b, extracapsular extension (EPE), seminal vesicle invasion (SVI), positive surgical margins (PSM) and Prostate Specific Antigen Density (PSAD) were all significantly associated with PSA persistence after RP (P < 0.05). In terms of surgical approach, RARP was considered a protective factor against postoperative PSA persistence (OR:0.53, p < 0.05). In multivariate logistic regression analysis, preoperative ISUP grade 4, percentage of positive cores and PSM were independent risk factors of PSA persistence after RP (P < 0.05).
Preoperative PSA, high-risk group, preoperative ISUP grades 2-5, postoperative ISUP grades 3-5, percentage of positive cores, cT3, ≥pT3b, EPE, SVI, PSM and PSAD were independent risk factors for PSA persistence in prostate cancer patients after RP. This provides assistance for early monitoring and treatment of patients at high risk of persistent PSA in clinical practice.
对于局限性前列腺癌,以根治性前列腺切除术(RP)为中心的综合治疗方法通常是其最佳选择。RP 术后 6 至 8 周内,通常可将前列腺特异性抗原(PSA)水平降低至 0.1ng/ml 以下。然而,在临床实践中,5%至 24%的患者在术后 6 至 8 周时 PSA≥0.1ng/ml,这种现象称为 PSA 持续存在。许多基于欧洲和美国数据的研究表明,PSA 持续存在与术后不良结局之间存在关联,并进一步分析了 PSA 持续存在的危险因素。然而,基于中国数据的相关研究仍然很少。
对 2016 年 7 月 15 日至 2022 年 8 月 31 日在浙江大学医学院附属第一医院接受 RP 的 1347 例前列腺癌患者进行回顾性研究。基于纳入标准,进行单因素和多因素 logistic 回归分析,以探讨 PSA 持续存在的独立危险因素。
在 826 例 RP 后的前列腺癌患者中,有 124 例出现 PSA 持续存在。在单因素 logistic 回归分析中,机器人辅助腹腔镜根治性前列腺切除术(RARP)、术前 PSA、高危组、术前国际泌尿病理学会(ISUP)分级 2-5、术后 ISUP 分级 3-5、阳性核心百分比、cT3、≥pT3b、包膜外侵犯(EPE)、精囊侵犯(SVI)、阳性手术切缘(PSM)和前列腺特异性抗原密度(PSAD)均与 RP 后 PSA 持续存在显著相关(P<0.05)。就手术方式而言,RARP 被认为是术后 PSA 持续存在的保护因素(OR:0.53,p<0.05)。多因素 logistic 回归分析显示,术前 ISUP 分级 4、阳性核心百分比和 PSM 是 RP 后 PSA 持续存在的独立危险因素(P<0.05)。
术前 PSA、高危组、术前 ISUP 分级 2-5、术后 ISUP 分级 3-5、阳性核心百分比、cT3、≥pT3b、EPE、SVI、PSM 和 PSAD 是 RP 后前列腺癌患者 PSA 持续存在的独立危险因素。这为临床实践中 PSA 持续存在风险较高的患者的早期监测和治疗提供了帮助。