Lax Stephanie J, Van Vogt Eleanor, Candy Bridget, Steele Lloyd, Reynolds Clare, Stuart Beth, Parker Roses, Axon Emma, Roberts Amanda, Doyle Megan, Chu Derek K, Futamura Masaki, Santer Miriam, Williams Hywel C, Cro Suzie, Drucker Aaron M, Boyle Robert J
Centre of Evidence Based Dermatology, University of Nottingham, Nottingham, UK.
Imperial Clinical Trials Unit, Imperial College London, London, UK.
Clin Exp Allergy. 2024 Dec;54(12):960-972. doi: 10.1111/cea.14556. Epub 2024 Sep 2.
Eczema is the most burdensome skin condition worldwide and topical anti-inflammatory treatments are commonly used to control symptoms. The relative effectiveness and safety of different topical anti-inflammatory treatments is uncertain.
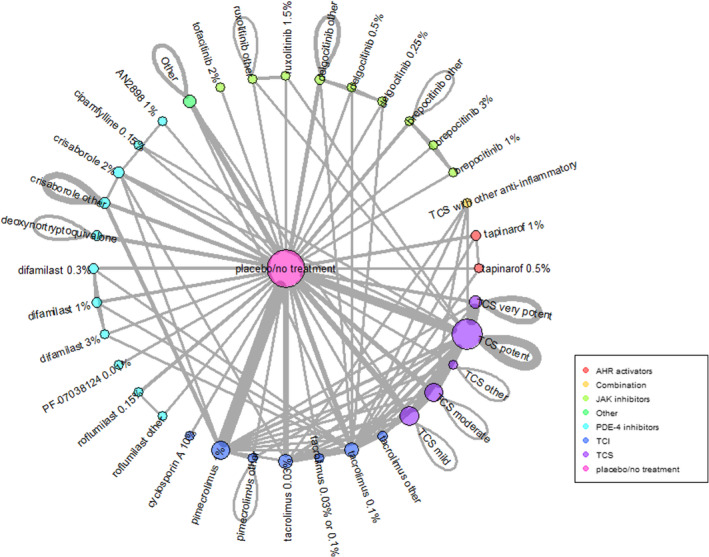
Network meta-analysis performed within a Cochrane systematic review to compare and statistically rank efficacy and safety of topical anti-inflammatory eczema treatments.
Cochrane Skin Specialised Register, CENTRAL, MEDLINE, Embase and trial registries to June 2023.
Included trials were within-participant or between-participant randomised controlled trials. Participants had eczema that was not clinically infected and was not contact dermatitis, seborrheic eczema or hand eczema. Interventions were topical anti-inflammatory treatments but not complementary treatments, antibiotics alone, wet wraps, phototherapy or systemic treatments. Comparators were no treatment/vehicle or another topical anti-inflammatory.
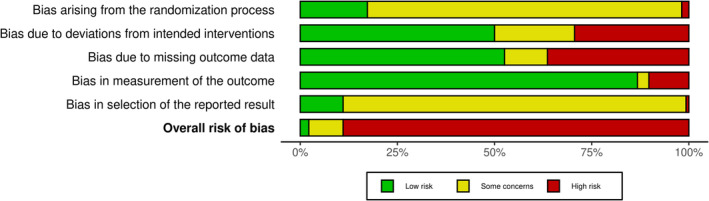
We identified 291 trials (45,846 participants), mainly in high-income countries. Most were industry-funded with median 3 weeks treatment duration. Risk of bias assessed using the Cochrane Risk of Bias 2.0 tool was high in 89% of trials, mainly due to risk of selective reporting. Network meta-analysis of binary outcomes ranked potent and/or very potent topical steroids, tacrolimus 0.1% and ruxolitinib 1.5% among the most effective treatments for improving patient-reported symptoms (40 trials, all low confidence) and clinician-reported signs (32 trials, all moderate confidence). For investigator global assessment, the Janus kinas inhibitors ruxolitinib 1.5%, delgocitinib 0.5% or 0.25%, very potent/potent topical steroids and tacrolimus 0.1% were ranked as most effective (140 trials, all moderate confidence). Continuous outcome data were mixed. Local application site reactions were most common with tacrolimus 0.1% (moderate confidence) and crisaborole 2% (high confidence) and least common with topical steroids (moderate confidence). Skin thinning was not increased with short-term use of any topical steroid potency (low confidence) but skin thinning was reported in 6/2044 (0.3%) participants treated with longer-term (6-60 months) topical steroids.
Potent topical steroids, Janus kinase inhibitors and tacrolimus 0.1% were consistently ranked as among the most effective topical anti-inflammatory treatments for eczema.
湿疹是全球最具负担的皮肤疾病,局部抗炎治疗常用于控制症状。不同局部抗炎治疗的相对有效性和安全性尚不确定。
在Cochrane系统评价中进行网络荟萃分析,以比较并对局部抗炎湿疹治疗的疗效和安全性进行统计学排序。
截至2023年6月的Cochrane皮肤专科注册库、CENTRAL、MEDLINE、Embase和试验注册库。
纳入的试验为参与者自身对照或参与者间随机对照试验。参与者患有非临床感染的湿疹,且不是接触性皮炎、脂溢性皮炎或手部湿疹。干预措施为局部抗炎治疗,但不包括辅助治疗、单独使用抗生素、湿敷、光疗或全身治疗。对照为不治疗/赋形剂或另一种局部抗炎药。
我们识别出291项试验(45846名参与者),主要来自高收入国家。大多数试验由行业资助,治疗持续时间中位数为3周。使用Cochrane偏倚风险2.0工具评估的偏倚风险在89%的试验中较高,主要是由于选择性报告风险。二元结局的网络荟萃分析将强效和/或超强效局部类固醇、0.1%他克莫司和1.5%芦可替尼列为改善患者报告症状(40项试验,均为低可信度)和临床医生报告体征(32项试验,均为中等可信度)最有效的治疗方法。对于研究者整体评估,Janus激酶抑制剂1.5%芦可替尼、0.5%或0.25%地尔戈替尼、超强效/强效局部类固醇和0.1%他克莫司被列为最有效(140项试验,均为中等可信度)。连续结局数据参差不齐。局部应用部位反应在0.1%他克莫司(中等可信度)和2%克立硼罗(高可信度)中最常见,在局部类固醇中最不常见(中等可信度)。短期使用任何强度的局部类固醇均未增加皮肤变薄风险(低可信度),但在接受长期(6 - 60个月)局部类固醇治疗的2044名参与者中有6名(0.3%)报告有皮肤变薄情况。
强效局部类固醇、Janus激酶抑制剂和0.1%他克莫司一直被列为湿疹最有效的局部抗炎治疗方法。