Department of Psychology, University of Otago, Dunedin, New Zealand.
School of Psychology, Charles Sturt University, Bathurst, NSW, Australia.
J Psychopharmacol. 2024 Sep;38(9):789-797. doi: 10.1177/02698811241275627. Epub 2024 Sep 2.
Anxiety and depression cause major detriment to the patient, family, and society - particularly in treatment-resistant (TR) cases, which are highly prevalent. TR prevalence may be due to current diagnoses being based not on biological measures but on symptom lists that suffer from clinical subjectivity, variation in symptom presentation, and comorbidity.
Goal-conflict-specific rhythmicity (GCSR) measured using the Stop-Signal Task (SST) may provide the first neural biomarker for an anxiety process and disorder. This GCSR has been validated with selective drugs for anxiety. So, we proposed that GCSR could differ between TR and non-TR individuals and do so differently between those diagnoses normally sensitive to selective anxiolytics and those not.
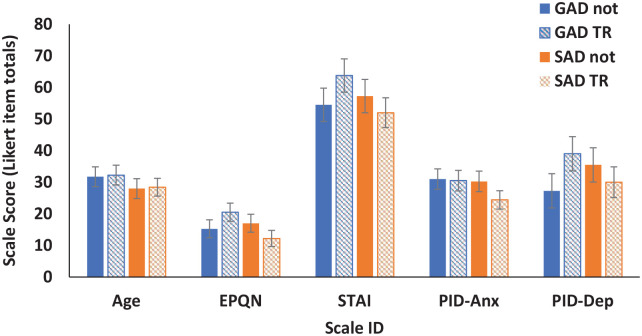
We recorded electroencephalograms (EEG) from 20 TR participants (4 GAD, 5 SAD and 11 MDD) and 24 non-TR participants (4 GAD, 5 SAD and 15 Comorbid GAD/MDD (GMD)) while they performed the SST.
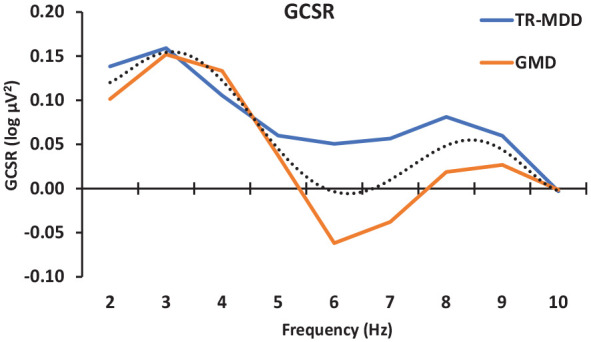
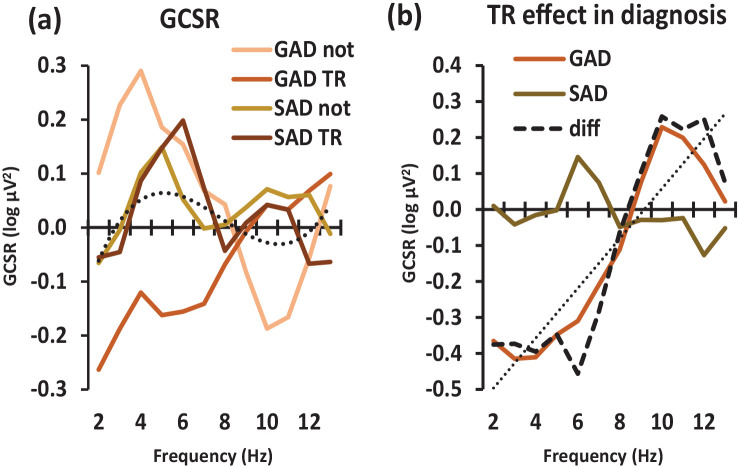
There was significant positive GCSR in all groups except the GAD-TR group. GAD-TR lacked GCSR in the low-frequency range. However, TR had little effect in SAD or MDD/GMD populations with apparent increases not decreases.
Overall, these results suggest that GAD may occur in two forms: one resulting from excessive GCSR and so being drug sensitive, and the other resulting from some other mechanism and so being TR. In SAD and MDD groups, heightened GCSR could be a consequence rather than the cause, driven by mechanisms that are normally more sensitive to non-selective panicolytic antidepressants.
焦虑和抑郁会给患者、家庭和社会带来严重的不良影响——尤其是在治疗抵抗(TR)的情况下,这种情况非常普遍。TR 的患病率可能是由于目前的诊断不是基于生物指标,而是基于症状清单,这些症状清单存在临床主观性、症状表现的变化和共病。
使用停止信号任务(SST)测量的目标冲突特异性节律性(GCSR)可能为焦虑过程和障碍提供第一个神经生物标志物。这种 GCSR 已经通过针对焦虑的选择性药物进行了验证。因此,我们提出 GCSR 可能在 TR 和非 TR 个体之间存在差异,并且在对选择性抗焦虑药物敏感和不敏感的诊断之间存在不同的差异。
我们记录了 20 名 TR 参与者(4 名 GAD、5 名 SAD 和 11 名 MDD)和 24 名非 TR 参与者(4 名 GAD、5 名 SAD 和 15 名共病 GAD/MDD(GMD))在执行 SST 时的脑电图(EEG)。
除了 GAD-TR 组外,所有组都存在显著的正 GCSR。GAD-TR 在低频范围内缺乏 GCSR。然而,TR 对 SAD 或 MDD/GMD 人群的影响很小,似乎是增加而不是减少。
总的来说,这些结果表明 GAD 可能有两种形式:一种是由于过度的 GCSR 而导致药物敏感,另一种是由于其他机制而导致 TR。在 SAD 和 MDD 组中,GCSR 的升高可能是一种后果,而不是原因,是由通常对非选择性抗惊恐和抗抑郁药物更敏感的机制驱动的。