Yong Loo Lin School of Medicine, National University of Singapore, National University Health System, Singapore, Singapore.
Australian and New Zealand Intensive Care Research Centre, Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, VIC, Australia.
Intensive Care Med. 2024 Nov;50(11):1861-1872. doi: 10.1007/s00134-024-07609-y. Epub 2024 Sep 2.
Acute hypoxaemic respiratory failure (AHRF) is a common reason for intensive care unit (ICU) admission. However, patient characteristics, outcomes, and trends over time are unclear. We describe the epidemiology and outcomes of patients with AHRF over time.
In this binational, registry-based study from 2005 to 2022, we included all adults admitted to an Australian or New Zealand ICU with an arterial blood gas within the first 24 h of ICU stay. AHRF was defined as a partial pressure of oxygen/inspired oxygen ratio (PaO/FiO) ≤ 300. The primary outcome was adjusted in-hospital mortality, categorised based on PaO/FiO (mild: 200-300, moderate: 100-200, and severe < 100, and non-linearly). We investigated how adjusted mortality evolved based on temporal trends (by year of admission), sex, age, admission diagnosis and the receipt of mechanical ventilation.
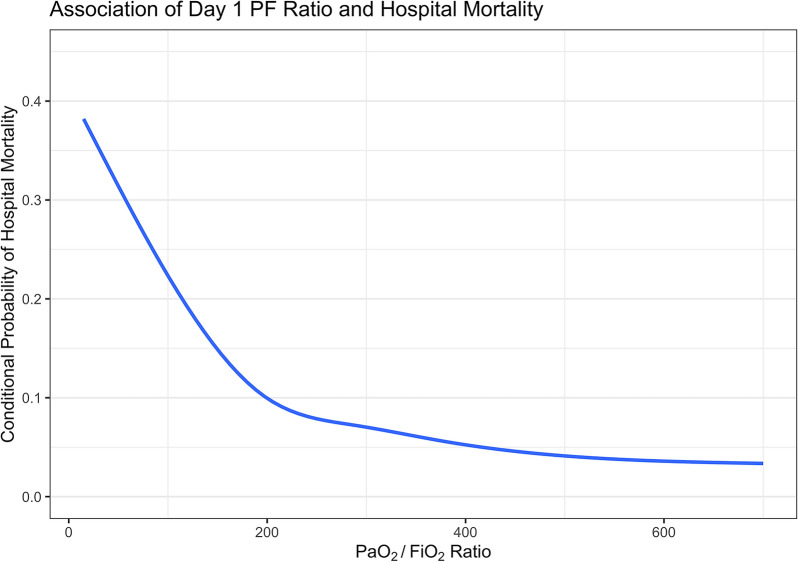
Of 1,560,221 patients, 826,106 (52.9%) were admitted with or developed AHRF within the first 24 h of ICU stay. Of these 826,106 patients, 51.4% had mild, 39.3% had moderate, and 9.3% had severe AHRF. Compared to patients without AHRF (5.3%), patients with mild (8%), moderate (14.2%) and severe (29.9%) AHRF had higher in-hospital mortality rates. As PaO/FiO ratio decreased, adjusted in-hospital mortality progressively increased, particularly below an inflection point at a PaO/FiO ratio of 200. The adjusted in-hospital mortality for all patients decreased over time (13.3% in 2005 to 8.2% in 2022), and this trend was similar in patients with and without AHRF.
The healthcare burden due to AHRF may be larger than expected, and mortality rates remain high in severe AHRF. Although mortality has decreased over time, this may reflect improvements in ICU care in general, rather than specifically in AHRF. More research is required to earlier identify AHRF and stratify these patients at risk of deterioration early, and to validate our findings.
急性低氧性呼吸衰竭(AHRF)是入住重症监护病房(ICU)的常见原因。然而,患者的特征、结局和随时间的变化趋势尚不清楚。我们描述了随时间变化 AHRF 患者的流行病学和结局。
在这项 2005 年至 2022 年的两国、基于登记的研究中,我们纳入了所有在入住 ICU 的头 24 小时内进行了动脉血气检查的澳大利亚或新西兰 ICU 成人患者。AHRF 定义为氧分压/吸入氧比值(PaO/FiO)≤300。主要结局是根据 PaO/FiO (轻度:200-300,中度:100-200,重度<100,呈非线性)调整的院内死亡率。我们调查了根据时间趋势(按入院年份)、性别、年龄、入院诊断和接受机械通气的情况,调整后的死亡率如何演变。
在 1560221 名患者中,826106 名(52.9%)在入住 ICU 的头 24 小时内入住或出现 AHRF。在这 826106 名患者中,51.4%为轻度,39.3%为中度,9.3%为重度。与无 AHRF 的患者(5.3%)相比,轻度(8%)、中度(14.2%)和重度(29.9%)AHRF 患者的院内死亡率更高。随着 PaO/FiO 比值的降低,调整后的院内死亡率逐渐升高,特别是在 PaO/FiO 比值低于 200 的拐点处。所有患者的调整后院内死亡率随时间而降低(2005 年的 13.3%降至 2022 年的 8.2%),且这种趋势在有和无 AHRF 的患者中相似。
AHRF 导致的医疗保健负担可能比预期的更大,重度 AHRF 的死亡率仍然很高。尽管死亡率随时间有所下降,但这可能反映了 ICU 整体护理的改善,而不仅仅是 AHRF 方面的改善。需要进一步研究以更早地识别 AHRF,并尽早对这些有恶化风险的患者进行分层,同时验证我们的研究结果。