Siebrecht Michael, Briaire Jeroen J, Verbist Berit M, Kalkman Randy K, Frijns Johan H M
Department of Otorhinolaryngology and Head & Neck Surgery, Leiden University Medical Center, PO Box 9600, 2300 RC, Leiden, the Netherlands.
Leiden Institute for Brain and Cognition, PO Box 9600, 2300 RC, Leiden, the Netherlands.
Heliyon. 2024 Aug 6;10(16):e35737. doi: 10.1016/j.heliyon.2024.e35737. eCollection 2024 Aug 30.
Knowledge of the cochlear anatomy in individual patients is helpful for improving electrode selection and placement during cochlear implantation, as well as in surgical planning. The aim of this study was to develop a model-free automated segmentation algorithm to obtain 3D surfaces from clinical computed tomography (CT) scans that describe an individual's cochlear anatomy and can be used to quantitatively analyze the cochlea's vertical trajectory.
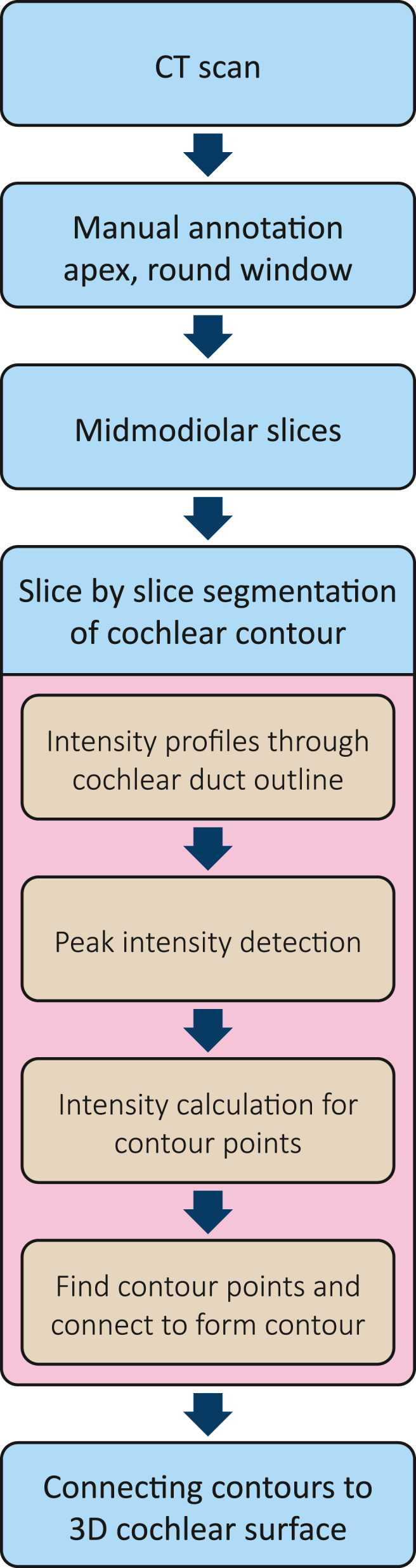
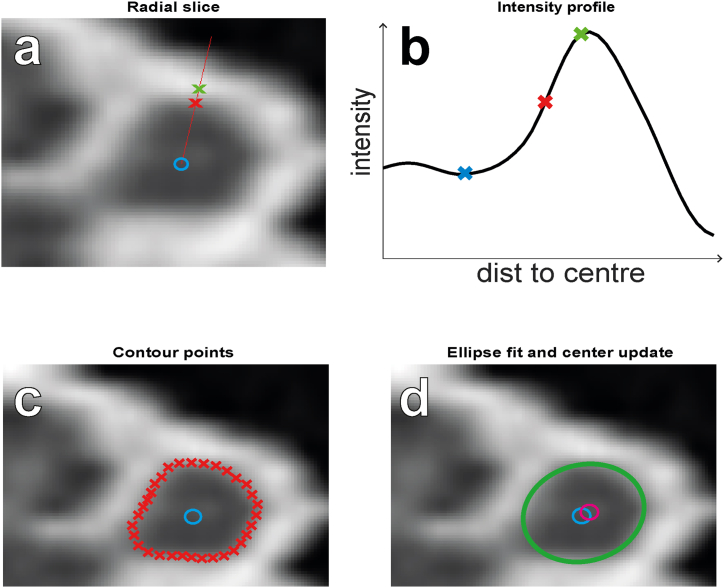
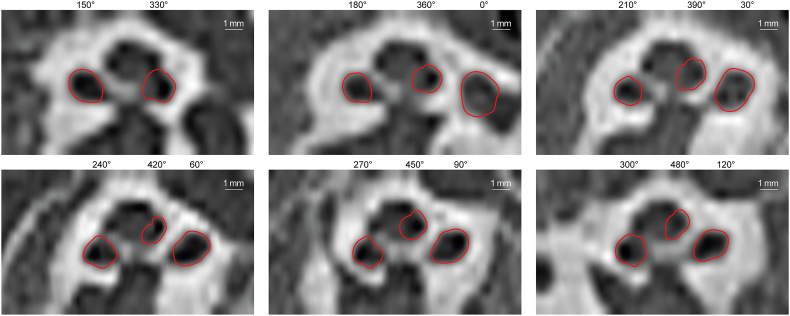
Clinical CT scans were re-oriented and re-sliced to obtain mid-modiolar slices. Using these slices, we segmented the cross-section of the cochlea.
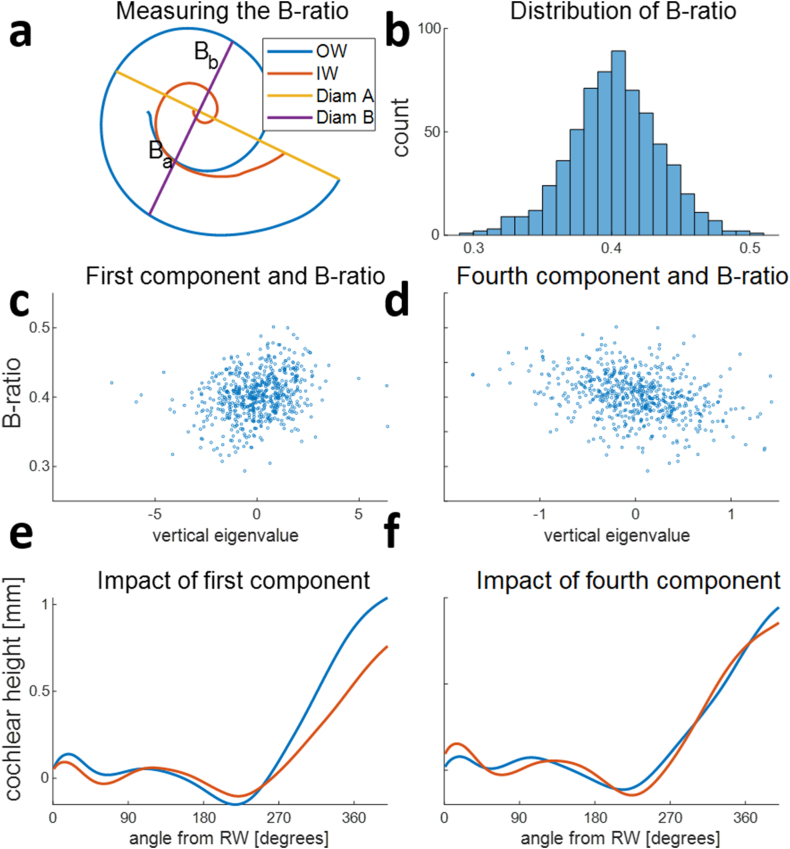
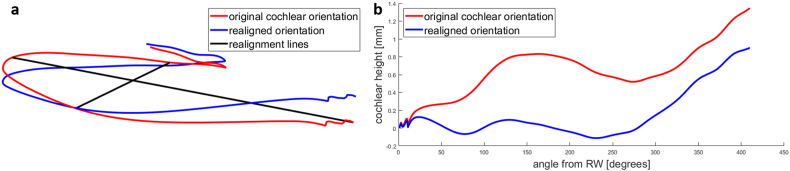
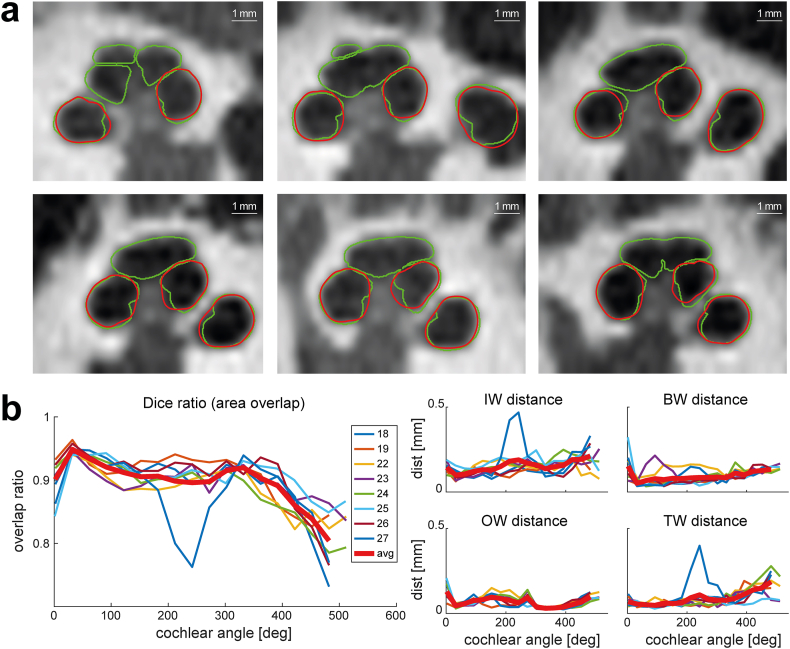
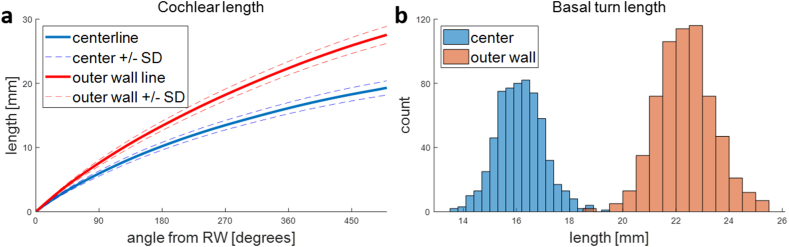
3D surfaces were obtained for the first 1.5 turns of 648 cochleae. Validation of our algorithm against the manually segmented ground truth obtained from 8 micro-CT scans showed good agreement, with 90 % area overlap and an average distance of 0.11 mm between the segmentation contours. The average cochlear duct length for the basal turn was 16.1 mm along the central path and 22.4 mm along the outer wall. The use of an intrinsic, observer-independent coordinate system and principal component analysis enabled unambiguous quantitative evaluation of the vertical trajectory of the cochlea, revealing only a weak correlation between the symmetry of the commonly used basal turn diameters (B-ratio of A and B diameters) and the profile of the vertical trajectory.
A model-free segmentation algorithm can achieve similar accuracy as previously published methods relying on statistical shapes. Quantitative analysis of the vertical trajectory can replace the categorization into rollercoaster, sloping, or intermediate vertical trajectory types.
了解个体患者的耳蜗解剖结构有助于在人工耳蜗植入过程中改进电极选择和放置,以及进行手术规划。本研究的目的是开发一种无模型自动分割算法,从临床计算机断层扫描(CT)中获取描述个体耳蜗解剖结构的三维表面,并可用于定量分析耳蜗的垂直轨迹。
对临床CT扫描进行重新定向和重新切片,以获得中轴切片。利用这些切片,我们对耳蜗的横截面进行了分割。
获得了648个耳蜗前1.5圈的三维表面。将我们的算法与从8次显微CT扫描中手动分割得到的真实情况进行验证,结果显示一致性良好,分割轮廓之间的面积重叠率为90%,平均距离为0.11毫米。基底转的耳蜗管平均长度沿中心路径为16.1毫米,沿外壁为22.4毫米。使用固有、与观察者无关的坐标系和主成分分析能够对耳蜗的垂直轨迹进行明确的定量评估,结果显示常用的基底转直径对称性(A和B直径的B比率)与垂直轨迹轮廓之间仅存在微弱相关性。
无模型分割算法可达到与先前发表的依赖统计形状的方法相似的准确性。对垂直轨迹的定量分析可取代将其分类为过山车型、倾斜型或中间垂直轨迹类型。