College of Medicine, The Ohio State University, Columbus, Ohio, United States of America.
Department of Anesthesiology, The Ohio State University Wexner Medical Center, Columbus, Ohio, United States of America.
PLoS One. 2024 Sep 4;19(9):e0309515. doi: 10.1371/journal.pone.0309515. eCollection 2024.
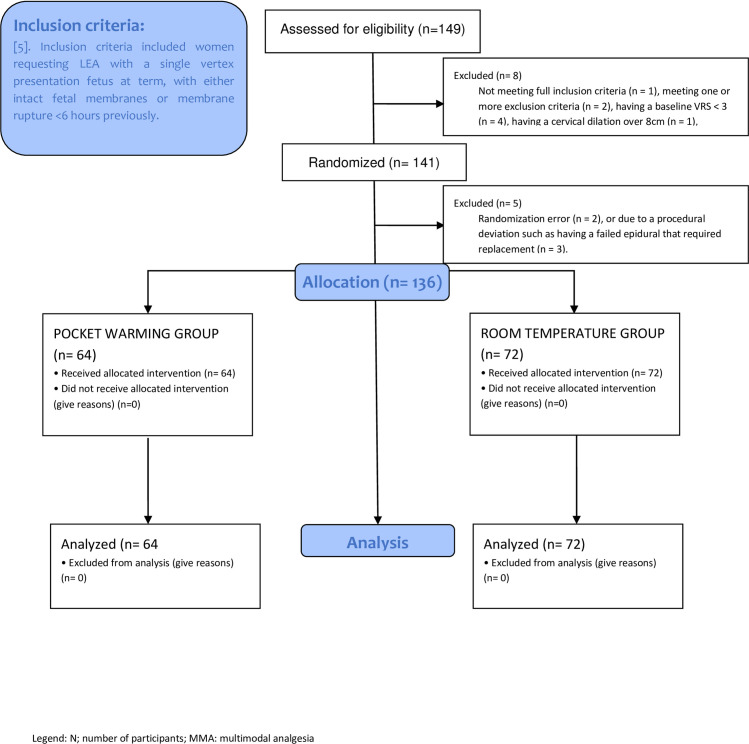
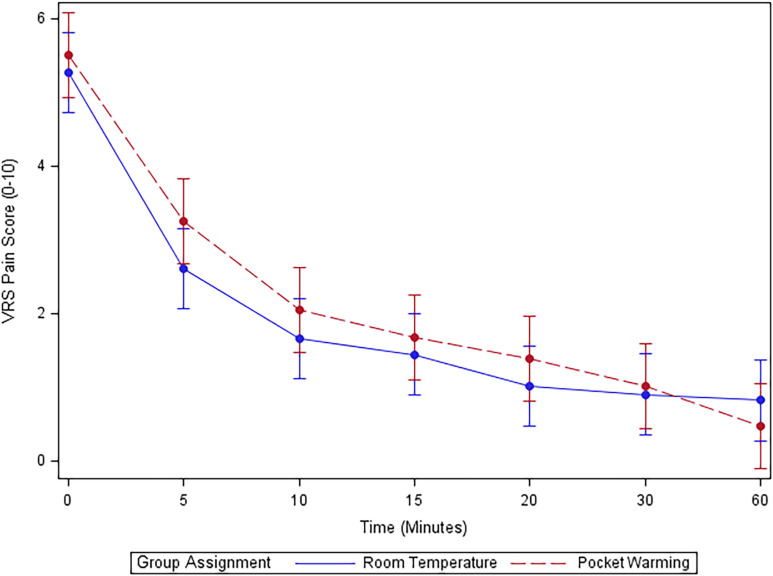
Shortening analgesic onset has been researched and it has been documented that prewarming epidural medications to body temperature (37°C) prior to administration increases medication efficacy. Our double-blind randomized controlled trial was designed to investigate if a lower degree of prewarming in providers' pockets could achieve similar results without the need of a bedside incubator. A total of 136 parturients were randomized into either the pocket-warmed group or the room temperature group to receive 10 mL of 0.125% bupivacaine with 2 μg/mL fentanyl epidural bolus at either the 27.8 ±1.7°C or 22.1 ±1.0°C temperatures, respectively. Primary outcome, time to analgesic onset (verbal rating scale pain score ≤ 3) was recorded in 0-, 5-, 10-, 15-, 20-, 30-, and 60-minutes intervals. It was observed that the pocket-warming group (n = 64) and room temperature group (n = 72) had no significant difference of analgesic onset time (median 8 vs. 6.2 minutes; p = 0.322). The incidence of adverse events such as hypotension, fever (≥ 38°C), nausea, vomiting, and number of top-off epidural boluses, as well as patient satisfaction rates and mode of delivery, were not significantly different between the groups as well. Further research is warranted to confirm these findings and explore the impact of different temperatures on analgesic onset time as well as the logistical issues associated with their clinical implementations.
缩短镇痛起效时间一直是研究的热点,已有文献证明,在给药前将硬膜外药物预热至体温(37°C)可提高药物疗效。我们的双盲随机对照试验旨在研究在没有床边孵化器的情况下,提供者口袋中较低程度的预加热是否可以达到类似的效果。共有 136 名产妇被随机分为口袋加热组或室温组,分别在 27.8±1.7°C 或 22.1±1.0°C 温度下接受 10 mL 0.125%布比卡因加 2μg/mL 芬太尼硬膜外推注。主要结局为镇痛起效时间(口述评分量表疼痛评分≤3),记录在 0、5、10、15、20、30 和 60 分钟的间隔时间内。结果显示,口袋加热组(n=64)和室温组(n=72)的镇痛起效时间无显著差异(中位数 8 分钟与 6.2 分钟;p=0.322)。两组的不良反应发生率(低血压、发热(≥38°C)、恶心、呕吐和硬膜外推注次数,以及患者满意度和分娩方式)也无显著差异。需要进一步研究来证实这些发现,并探讨不同温度对镇痛起效时间的影响,以及与临床实施相关的后勤问题。