Division of Respirology, Neurology, and Rheumatology, Department of Internal Medicine, Kurume University School of Medicine, 67 Asahi-Machi, Kurume, Fukuoka, 830-0011, Japan.
Biostatistics Center, Kurume University School of Medicine, Fukuoka, Japan.
Cancer Immunol Immunother. 2024 Sep 5;73(11):214. doi: 10.1007/s00262-024-03781-8.
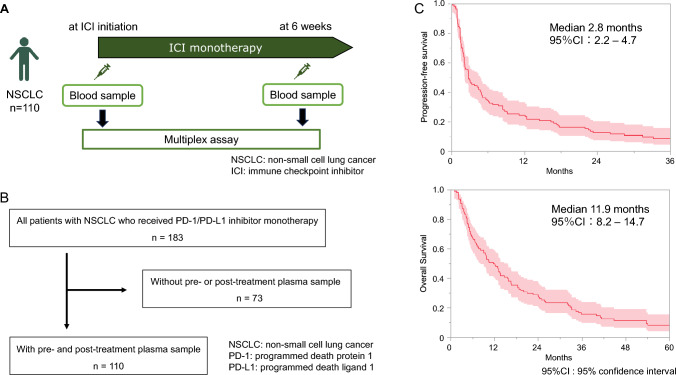
Despite the favorable therapeutic efficacy observed with ICI monotherapy, the majority of non-small cell lung cancer (NSCLC) patients do not respond. Therefore, identifying patients who could optimally benefit from ICI treatment remains a challenge.
Among 183 patients with advanced or recurrent NSCLC who received ICI monotherapy, we analyzed 110 patients whose pre- and post-treatment plasma samples were available. Seventy-three soluble immune mediators were measured at ICI initiation and 6 weeks later. To identify useful biomarkers, we analyzed the association of pre-treatment levels and on-treatment changes of soluble immune mediators with survival of patients. The associations of pre-treatment or on-treatment biomarkers with irAE development, PD-L1 expression, CD8+ TIL density, and neutrophil to lymphocyte ratio (NLR) were also analyzed.
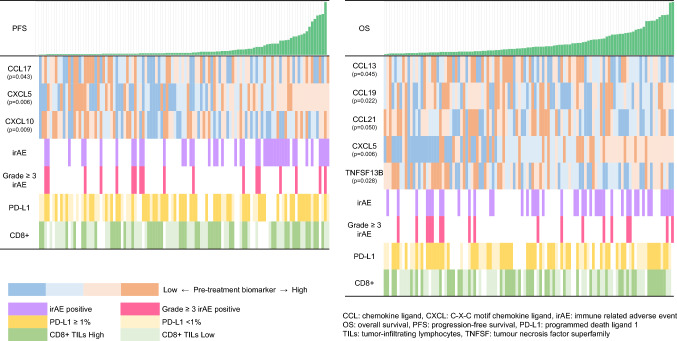
Univariate analysis showed that pre-treatment biomarkers included 6 immune mediators, whereas on-treatment biomarkers included 8 immune mediators. Multivariate analysis showed that pre-treatment biomarkers included 4 immune mediators (CCL19, CCL21, CXCL5, CXCL10), whereas on-treatment biomarkers included 5 immune mediators (CCL7, CCL19, CCL23, CCL25, IL-32). IrAE development was associated with on-treatment change in CCL23. PD-L1 expression was associated with the pre-treatment levels of TNFSF13B and the on-treatment change in CCL25. CD8+ TIL density was associated with the pre-treatment CXCL10 level, whereas NLR was correlated with pre-treatment levels of CCL13 and CCL17.
We identified several soluble immune mediators as pre-treatment and on-treatment biomarkers of survival in patients with NSCLC treated with ICI monotherapy. Some of these biomarkers were associated with other possible predictors, including irAE development, PD-L1 expression, CD8+ TIL density and NLR. Further large-scale studies are needed to establish biomarkers for patients with NSCLC who received ICI monotherapy.
尽管免疫检查点抑制剂(ICI)单药治疗具有良好的疗效,但大多数非小细胞肺癌(NSCLC)患者对此无反应。因此,确定哪些患者能从 ICI 治疗中获益最大仍然是一个挑战。
在 183 例接受 ICI 单药治疗的晚期或复发性 NSCLC 患者中,我们分析了 110 例有治疗前后血浆样本的患者。在 ICI 起始时和 6 周后检测了 73 种可溶性免疫介质。为了确定有用的生物标志物,我们分析了治疗前水平和治疗过程中可溶性免疫介质的变化与患者生存的关系。还分析了治疗前或治疗中生物标志物与免疫相关不良事件(irAE)的发生、PD-L1 表达、CD8+TIL 密度和中性粒细胞与淋巴细胞比值(NLR)之间的关系。
单因素分析显示,治疗前的生物标志物包括 6 种免疫介质,而治疗中的生物标志物包括 8 种免疫介质。多因素分析显示,治疗前的生物标志物包括 4 种免疫介质(CCL19、CCL21、CXCL5、CXCL10),而治疗中的生物标志物包括 5 种免疫介质(CCL7、CCL19、CCL23、CCL25、IL-32)。irAE 的发生与 CCL23 的治疗中变化有关。PD-L1 表达与 TNFSF13B 的治疗前水平和 CCL25 的治疗中变化有关。CD8+TIL 密度与治疗前 CXCL10 水平有关,而 NLR 与 CCL13 和 CCL17 的治疗前水平有关。
我们确定了一些可溶性免疫介质作为 NSCLC 患者接受 ICI 单药治疗的生存的治疗前和治疗中的生物标志物。其中一些生物标志物与其他可能的预测因子有关,包括 irAE 的发生、PD-L1 表达、CD8+TIL 密度和 NLR。需要进一步的大规模研究来为接受 ICI 单药治疗的 NSCLC 患者建立生物标志物。