McCracken Celeste, Condurache Dorina-Gabriela, Szabo Liliana, Elghazaly Hussein, Walter Fiona M, Mead Adam J, Chakraverty Ronjon, Harvey Nicholas C, Manisty Charlotte H, Petersen Steffen E, Neubauer Stefan, Raisi-Estabragh Zahra
Division of Cardiovascular Medicine, Radcliffe Department of Medicine, University of Oxford, National Institute for Health Research Oxford Biomedical Research Centre, Oxford University Hospitals NHS Foundation Trust, Oxford, United Kingdom.
Barts Heart Centre, St Bartholomew's Hospital, Barts Health NHS Trust, West Smithfield, London, United Kingdom.
JACC CardioOncol. 2024 Jul 23;6(4):575-588. doi: 10.1016/j.jaccao.2024.05.015. eCollection 2024 Aug.
Cardiovascular preventive strategies are guided by risk scores with unknown validity in cancer cohorts.
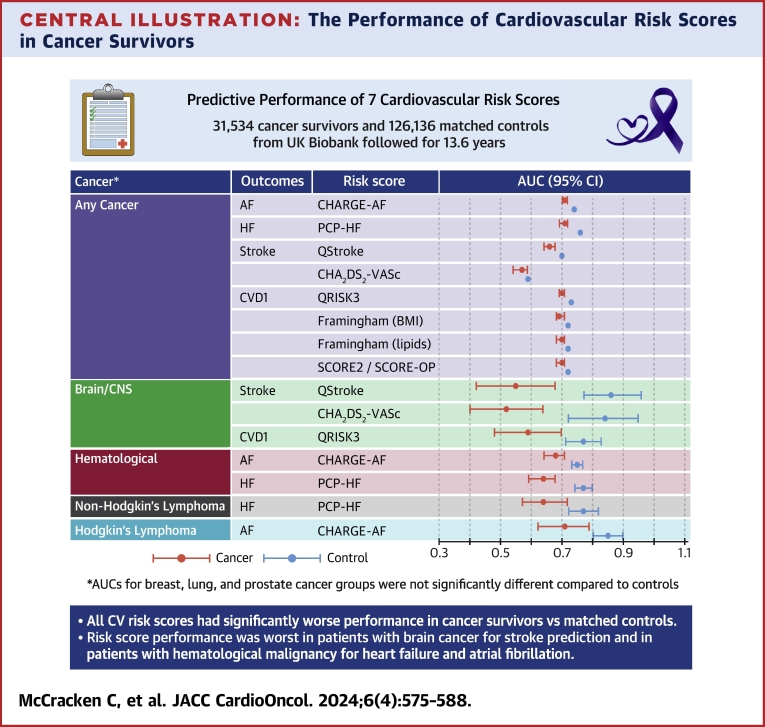
This study aimed to evaluate the predictive performance of 7 established cardiovascular risk scores in cancer survivors from the UK Biobank.
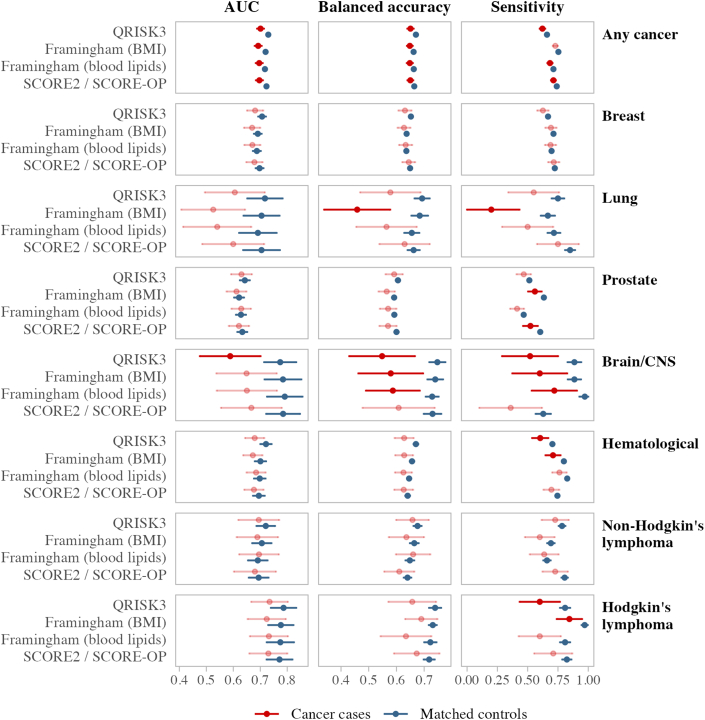
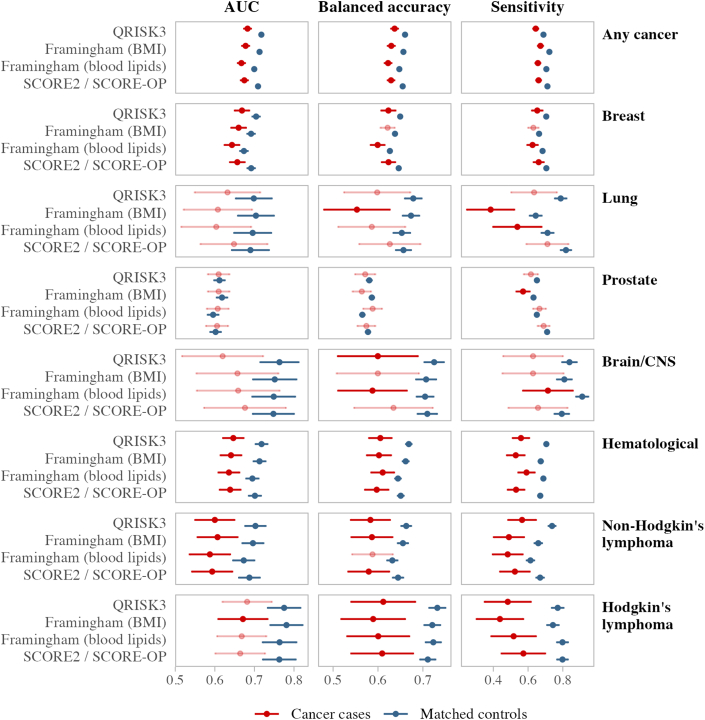
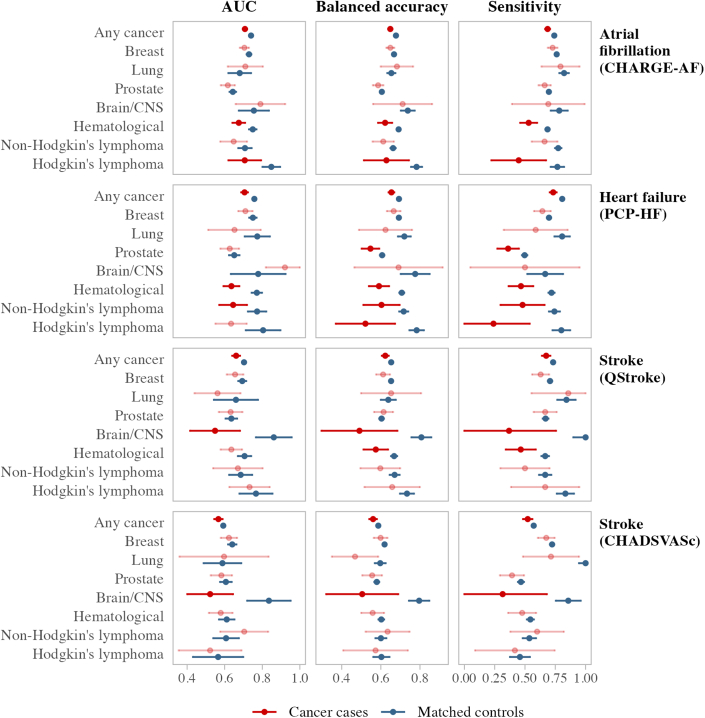
The predictive performance of QRISK3, Systematic Coronary Risk Evaluation 2 (SCORE2)/Systematic Coronary Risk Evaluation for Older Persons (SCORE-OP), Framingham Risk Score, Pooled Cohort equations to Prevent Heart Failure (PCP-HF), CHARGE-AF, QStroke, and CHADS-VASc was calculated in participants with and without a history of cancer. Participants were propensity matched on age, sex, deprivation, health behaviors, family history, and metabolic conditions. Analyses were stratified into any cancer, breast, lung, prostate, brain/central nervous system, hematologic malignancies, Hodgkin lymphoma, and non-Hodgkin lymphoma. Incident cardiovascular events were tracked through health record linkage over 10 years of follow-up. The area under the receiver operating curve, balanced accuracy, and sensitivity were reported.
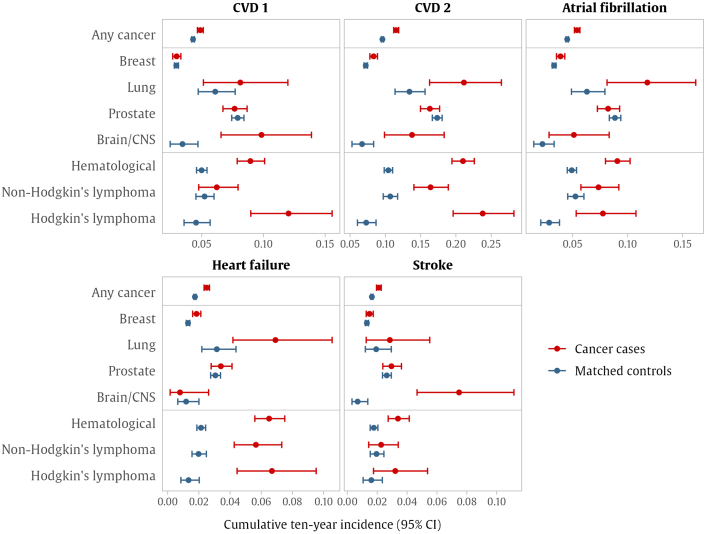
The analysis included 31,534 cancer survivors and 126,136 covariate-matched controls. Risk score distributions were near identical in cases and controls. Participants with any cancer had a significantly higher incidence of all cardiovascular outcomes than matched controls. Performance metrics were significantly worse for all risk scores in cancer cases than in matched controls. The most notable differences were among participants with a history of hematologic malignancies who had significantly higher outcome rates and poorer risk score performance than their matched controls. The performance of risk scores for predicting stroke in participants with brain/central nervous system cancer was very poor, with predictive accuracy more than 30% lower than noncancer controls.
Existing cardiovascular risk scores have significantly worse predictive accuracy in cancer survivors compared with noncancer comparators, leading to an underestimation of risk in this cohort.
心血管预防策略以风险评分作为指导,但这些评分在癌症队列中的有效性尚不清楚。
本研究旨在评估7种既定的心血管风险评分在英国生物银行癌症幸存者中的预测性能。
在有和没有癌症病史的参与者中计算QRISK3、系统性冠状动脉风险评估2(SCORE2)/老年人系统性冠状动脉风险评估(SCORE-OP)、弗雷明汉风险评分、预防心力衰竭的合并队列方程(PCP-HF)、CHARGE-AF、QStroke和CHADS-VASc的预测性能。参与者在年龄、性别、贫困程度、健康行为、家族病史和代谢状况方面进行倾向匹配。分析被分层为任何癌症、乳腺癌、肺癌、前列腺癌、脑/中枢神经系统癌、血液系统恶性肿瘤、霍奇金淋巴瘤和非霍奇金淋巴瘤。通过健康记录链接在10年的随访中跟踪心血管事件的发生情况。报告了受试者工作曲线下面积、平衡准确性和敏感性。
分析包括31,534名癌症幸存者和126,136名协变量匹配的对照。病例组和对照组的风险评分分布几乎相同。任何癌症患者的所有心血管结局发生率均显著高于匹配的对照组。癌症病例中所有风险评分的性能指标均显著低于匹配的对照组。最显著的差异出现在有血液系统恶性肿瘤病史的参与者中,他们的结局发生率显著更高,风险评分性能比匹配的对照组更差。脑/中枢神经系统癌症患者中预测中风的风险评分性能非常差,预测准确性比非癌症对照组低30%以上。
与非癌症对照相比,现有的心血管风险评分在癌症幸存者中的预测准确性显著更差,导致该队列中的风险被低估。