Soh Cheng Hwee, Marwick Thomas H
Imaging Research Laboratory, Baker Heart and Diabetes Institute, Melbourne, Australia.
Baker Department of Cardiometabolic Health, University of Melbourne, PO Box 6492, Melbourne, Victoria, 3004, Australia.
Cardiooncology. 2024 Oct 11;10(1):67. doi: 10.1186/s40959-024-00267-5.
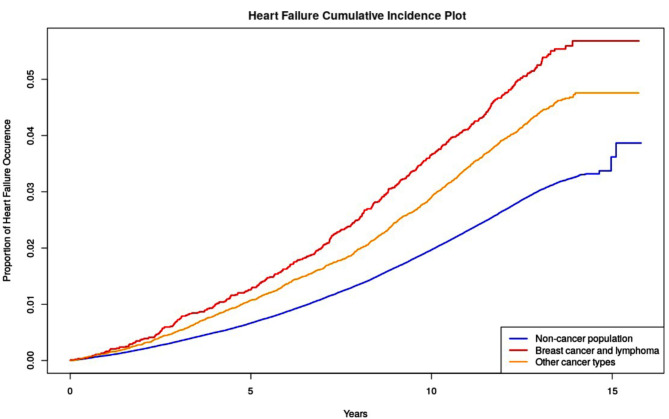
Cancer survivors have an increased risk of incident heart failure (HF) attributable to shared risk factors and cancer treatment-induced cardiac dysfunction. Selection for HF screening depends on risk assessment, but the optimal means of assessing risk is undefined. We undertook a comparison of HF risk calculators among survivors.
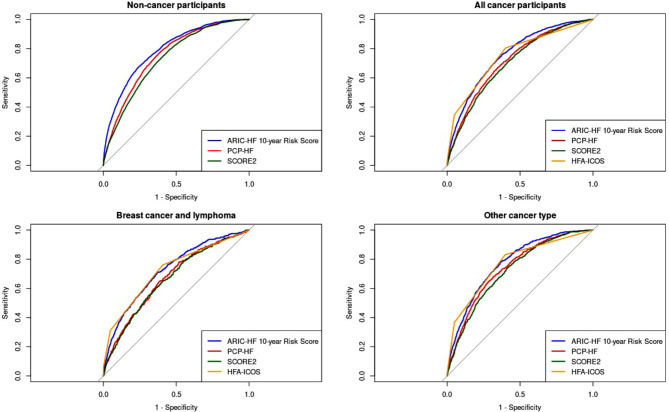
In this study from the UK Biobank, cancer and HF diagnoses were determined based on the International Classification of Diseases (ICD)-10 code and non-cancer participants were included as controls. Participants' risk of incident HF was determined using the Heart Failure Association-International Cardio-oncology Society (HFA-ICOS), the Atherosclerosis Risk in Communities (ARIC-HF) and the Pooled Cohort Equations to Prevent Heart Failure (PCP-HF). The predictive performances of each were compared using the area under the curve (AUC).
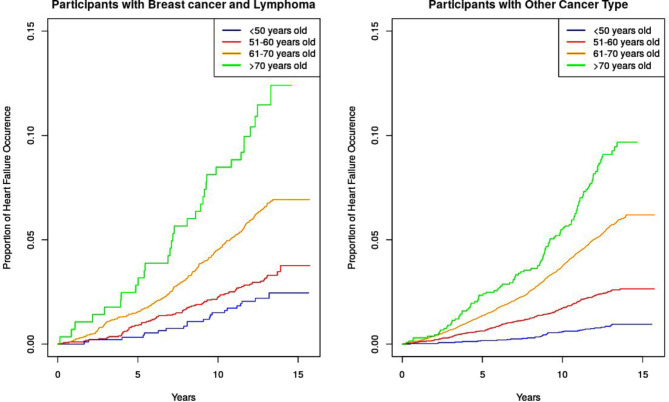
After propensity matching with age and sex, 9,232 survivors from breast cancer or lymphoma (mean age 59.9 years, 87.8% female), and 23,800 survivors from other cancer types (mean age 59.1 years, 85.8% female) were included in the analysis. The discriminative value for HFA-ICOS (AUC 0.753 [95%CI: 0.739-0.766]) and ARIC-HF (0.757 [95%CI: 0.744-0.770]) were similar, and superior to PCP-HF (0.717 [95%CI: 0.702-0.732]). The overall performance for each risk score was better among participants in other cancer types than those with breast cancer and lymphoma.
HFA-ICOS and ARIC-HF outperformed the PCP-HF among cancer- and non-cancer cohort, although all showed modest discrimination for incident HF to be applied to clinical practice. A cancer-specific HF prediction tool could facilitate HF prevention among survivors.
癌症幸存者因共同的风险因素和癌症治疗引起的心脏功能障碍,发生心力衰竭(HF)的风险增加。HF筛查的选择取决于风险评估,但评估风险的最佳方法尚未明确。我们对幸存者中的HF风险计算器进行了比较。
在这项来自英国生物银行的研究中,根据国际疾病分类(ICD)-10编码确定癌症和HF诊断,并将非癌症参与者作为对照。使用心力衰竭协会-国际心脏肿瘤学会(HFA-ICOS)、社区动脉粥样硬化风险(ARIC-HF)和预防心力衰竭合并队列方程(PCP-HF)确定参与者发生HF的风险。使用曲线下面积(AUC)比较每种方法的预测性能。
在按年龄和性别进行倾向匹配后,分析纳入了9232名乳腺癌或淋巴瘤幸存者(平均年龄59.9岁,女性占87.8%)和23800名其他癌症类型的幸存者(平均年龄59.1岁,女性占85.8%)。HFA-ICOS(AUC 0.753 [95%CI:0.739-0.766])和ARIC-HF(0.757 [95%CI:0.744-0.770])的判别值相似,且优于PCP-HF(0.717 [95%CI:0.702-0.732])。每种风险评分在其他癌症类型参与者中的总体表现优于乳腺癌和淋巴瘤患者。
在癌症和非癌症队列中,HFA-ICOS和ARIC-HF的表现优于PCP-HF,尽管所有方法对HF发生的判别能力在应用于临床实践时都较为有限。一种针对癌症的HF预测工具可能有助于预防幸存者发生HF。