Bierbrier Jared, Gerstein Emily, Whitmore George A, Vandemheen Katherine L, Bergeron Celine, Boulet Louis-Philippe, Cote Andreanne, Field Stephen K, Penz Erika, McIvor R Andrew, Lemière Catherine, Gupta Samir, Hernandez Paul, Mayers Irvin, Bhutani Mohit, Lougheed M Diane, Licskai Christopher J, Azher Tanweer, Ezer Nicole, Ainslie Martha, Alvarez Gonzalo G, Mulpuru Sunita, Aaron Shawn D
The Ottawa Hospital Research Institute, University of Ottawa, Ottawa, ON, Canada.
Desautels Faculty of Management, McGill University, Montreal, QC, Canada.
Chest. 2024 Dec;166(6):1296-1308. doi: 10.1016/j.chest.2024.07.183. Epub 2024 Sep 4.
We investigated dyspnea; its associated risk factors; and its impact on health care utilization, quality of life, and work productivity in adults with undiagnosed respiratory symptoms.
What is the impact of dyspnea in adults with undiagnosed respiratory symptoms?
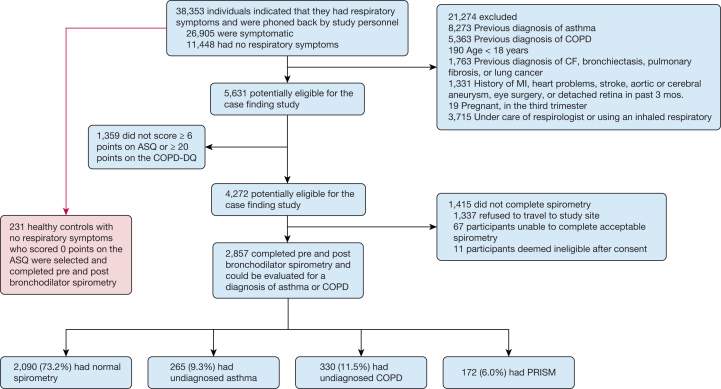
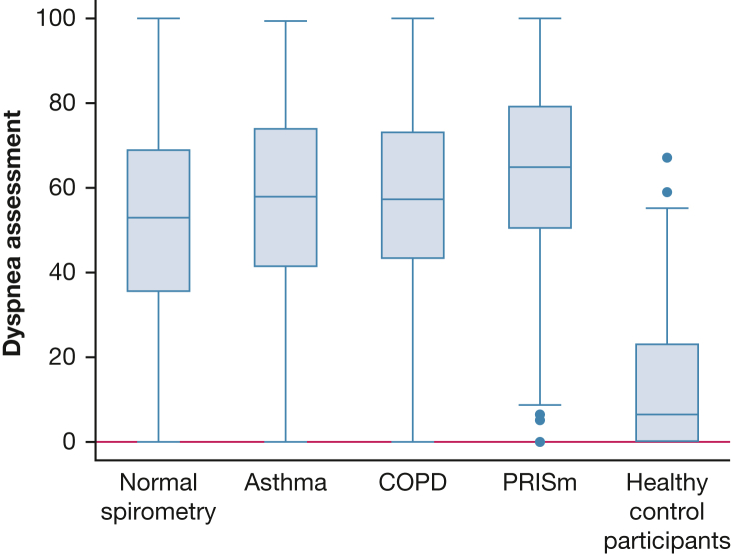
This population-based study included 2,857 adults who were experiencing respiratory symptoms. These individuals had not been previously diagnosed with any lung conditions and were recruited from 17 Canadian centers using random digit dialing. Each participant underwent spirometry testing both before and after using a bronchodilator to determine if they met the diagnostic criteria for COPD, asthma, or preserved ratio impaired spirometry (PRISm), or if their spirometry results were normal. An age-matched control group (n = 231) was similarly recruited using random digit dialing. A dyspnea impact assessment score from 0 to 100 was produced using questions from the COPD Assessment Test and St. George's Respiratory questionnaire.
Individuals with PRISm (n = 172) reported more impactful dyspnea (mean score, 63.0; 95% CI, 59.5-66.4) than those with undiagnosed asthma (n = 265; mean score, 56.6; 95% CI, 53.9-59.3) or undiagnosed COPD (n = 330; mean score, 57.5; 95% CI, 55.1-59.9). All groups reported significantly more impactful dyspnea than the control group (mean score, 13.8; 95% CI, 11.8-15.7). Patient-specific risk factors including age, sex, BMI, smoking, and comorbidities explained 20.6% of the variation in dyspnea. An additional 12.4% of the variation was explained by disease classification and another 1.7% by the severity of lung function impairment assessed with spirometry. After adjusting for age, sex, and BMI, greater dyspnea impact was associated with increased health care utilization, lower quality of life, and reduced work productivity.
Our findings showed that in community-based adults with undiagnosed respiratory symptoms, those identified with PRISm experienced the greatest impact of dyspnea. Dyspnea imposes burdens on the health care system and is associated with impaired quality of life and work productivity.
我们调查了呼吸困难;其相关危险因素;以及它对有未确诊呼吸道症状的成年人的医疗保健利用、生活质量和工作生产力的影响。
呼吸困难对有未确诊呼吸道症状的成年人有何影响?
这项基于人群的研究纳入了2857名有呼吸道症状的成年人。这些个体此前未被诊断出患有任何肺部疾病,通过随机数字拨号从加拿大17个中心招募而来。每位参与者在使用支气管扩张剂前后均接受了肺活量测定测试,以确定他们是否符合慢性阻塞性肺疾病(COPD)、哮喘或肺功能保留比例受损(PRISm)的诊断标准,或者其肺活量测定结果是否正常。使用随机数字拨号以类似方式招募了一个年龄匹配的对照组(n = 231)。使用慢性阻塞性肺疾病评估测试和圣乔治呼吸问卷中的问题得出了一个从0到100的呼吸困难影响评估分数。
患有PRISm的个体(n = 172)报告的呼吸困难影响比未确诊哮喘的个体(n = 265;平均分数,56.6;95%可信区间,53.9 - 59.3)或未确诊COPD的个体(n = 330;平均分数,57.5;95%可信区间,55.1 - 59.9)更大。所有组报告的呼吸困难影响均显著高于对照组(平均分数,13.8;95%可信区间,11.8 - 15.7)。包括年龄、性别、体重指数、吸烟和合并症在内的患者特异性危险因素解释了呼吸困难变异的20.6%。疾病分类又解释了另外12.4%的变异,通过肺活量测定评估的肺功能损害严重程度解释了1.7%的变异。在对年龄、性别和体重指数进行调整后,更大的呼吸困难影响与医疗保健利用增加、生活质量降低和工作生产力下降相关。
我们的研究结果表明,在有未确诊呼吸道症状的社区成年人中,被确定患有PRISm的个体经历的呼吸困难影响最大。呼吸困难给医疗保健系统带来负担,并与生活质量受损和工作生产力下降相关。