Talahma Imad Ibrahim, Zawahra Aya Khader, Almakhtoob Falasteen Jameel, Shawar Fatima Iyad, Sharabati Khulood Marwan, Dwaik Raghad Faisal, Abdelshafy Marwa K, Farag Ahmed Adel, AbuAyyash Ahmad M, Hamouda Waeel O
Department of Neurosurgery, Al-Helal Hospital, Hebron, Palestinian Territory Occupied.
Medical Student, Faculty of Medicine, Palestine Polytechnic University, Hebron, Palestinian Territory Occupied.
Surg Neurol Int. 2024 Aug 9;15:275. doi: 10.25259/SNI_248_2024. eCollection 2024.
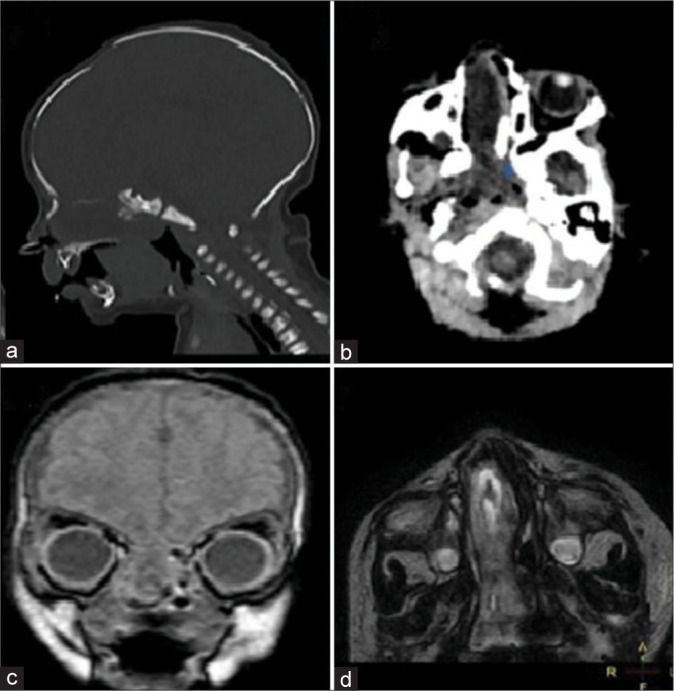
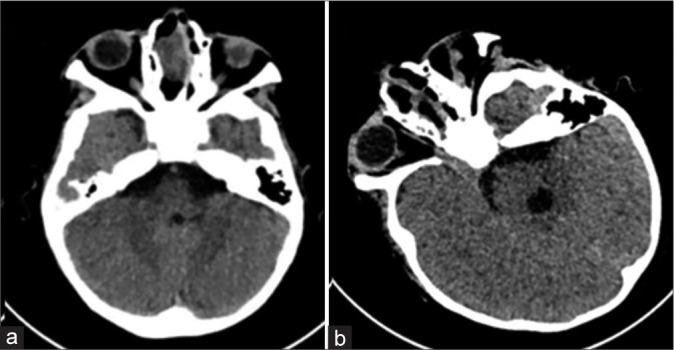
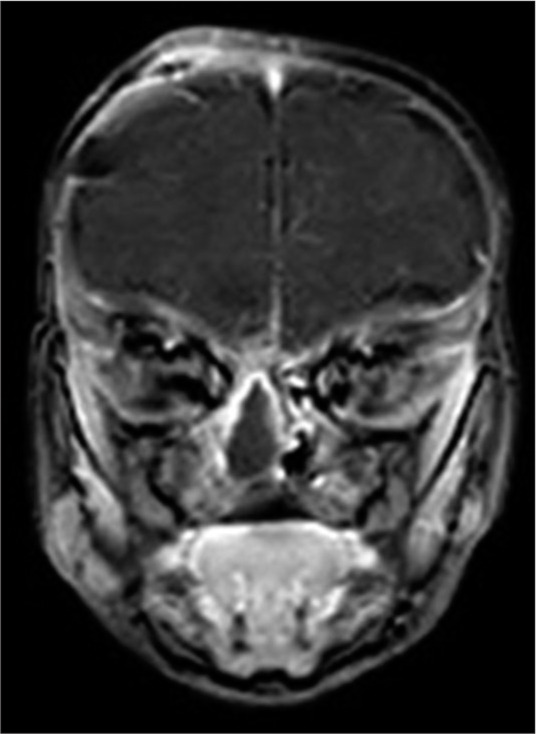
Intranasal meningoencephaloceles are rarely encountered in pediatric neurosurgery. The symptoms and clinical features may mimic those of nasal polyps or dermoid cysts. Transethmoidal meningoencephalocele is a rare congenital meningoencephalocele of the anterior skull base with diverse clinical presentation. The appropriate surgical intervention is chosen according to the meningoencephalocele type and location. Radiological examinations such as computed tomography and magnetic resonance imaging are helpful for the differential diagnosis of the encephalocele sac and localization of the cranial bone defect.
We are reporting a case of basal meningoencephalocele of the transethmoidal type, which was discovered in a 20-day-old boy presenting with cerebrospinal fluid rhinorrhea, respiratory distress, difficulty in feeding, and meningitis. The preoperative images showed a large herniated intranasal sac with bony discontinuity of the cribriform plate; however, three discrete defects of the cribriform plate with their related discrete herniated sacs were identified intraoperatively. Two staged surgeries were performed in succession: transcranial to separate the sacs from the cranial cavity and seal the anterior fossa floor, followed by transnasal to remove the remnant of the intranasal sacs. Patient symptoms and signs markedly improved after the surgeries.
We highlight the need for urgent intervention at a very young age if the clinical presentation mandates, and also the importance of meticulous intraoperative identification of all bony and dural defects that might be missed in preoperative images to ensure complete repair and prevent recurrence.
小儿神经外科中鼻内脑膜脑膨出很少见。其症状和临床特征可能与鼻息肉或皮样囊肿相似。经筛窦脑膜脑膨出是一种罕见的先天性前颅底脑膜脑膨出,临床表现多样。根据脑膜脑膨出的类型和位置选择合适的手术干预。计算机断层扫描和磁共振成像等影像学检查有助于脑膨出囊的鉴别诊断和颅骨缺损的定位。
我们报告一例经筛窦型基底脑膜脑膨出病例,该病例发现于一名20日龄男婴,表现为脑脊液鼻漏、呼吸窘迫、喂养困难和脑膜炎。术前影像显示鼻腔内有一个大的疝出囊,筛板骨质连续性中断;然而,术中发现筛板有三个离散的缺损及其相关的离散疝出囊。连续进行了两期手术:经颅将囊与颅腔分离并封闭前颅窝底,然后经鼻切除鼻腔内囊的残余部分。术后患者症状和体征明显改善。
我们强调,如果临床表现需要,在患儿很小的时候就需要紧急干预,同时强调术中仔细识别术前影像可能遗漏的所有骨质和硬脑膜缺损的重要性,以确保完全修复并防止复发。